


Summary
Alcohol, sometimes referred to by the chemical name ethanol, is a depressant drug found in fermented beverages such as beer, wine, and distilled spirit[11] -- in particular, rectified spirit.[12] Ethanol is colloquially refereed to as "alcohol" because it is the most prevalent alcohol in alcoholic beverages, but technically all alcoholic beverages contain several types of psychoactive alcohols, that are categorized as primary, secondary, or tertiary; Primary alcohols are oxidized to aldehydes, secondary alcohols undergo oxidation to form ketones, while tertiary alcohols are generally resistant to oxidation;[13] Ethanol is a primary alcohol that has unpleasant actions in the body, many of which are mediated by its toxic metabolite acetaldehyde.[14] Less prevalent alcohols found in alcoholic beverages, are secondary, and tertiary alcohols. For example, the tertiary alcohol 2M2B which is up to 50 times more potent than ethanol and found in trace quantities in alcoholic beverages, has been synthesized and used as a designer drug. Alcoholic beverages are sometimes laced with toxic alcohols, such as methanol (the simplest alcohol) and isopropyl alcohol.[11] A mild, brief exposure to isopropyl alcohol (which is only moderately more toxic than ethanol) is unlikely to cause any serious harm, but many methanol poisoning incidents have occurred through history, since methanol is lethal even in small quantities, as little as 10–15 milliliters (2–3 teaspoons). Ethanol is used to treat methanol and ethylene glycol toxicity.
 | |||
| |||
| Clinical data | |||
|---|---|---|---|
| Pronunciation | /ˈɛθənɒl/ | ||
| Other names | Absolute alcohol; Alcohol (USP); Cologne spirit; Drinking alcohol; Ethanol (JAN); Ethylic alcohol; EtOH; Ethyl alcohol; Ethyl hydrate; Ethyl hydroxide; Ethylol; Grain alcohol; Hydroxyethane; Methylcarbinol | ||
| Pregnancy category |
| ||
| Dependence liability | Physical: Very High Psychological: Moderate[1] | ||
| Addiction liability | Moderate (10–15%)[2] | ||
| Routes of administration | Common: Oral Uncommon: suppository, inhalation, ocular, insufflation, injection[3] | ||
| Drug class | Analgesic; Anxiolytic; Depressant; Euphoriant; GABAA receptor positive modulators; Sedative | ||
| ATC code |
| ||
| Legal status | |||
| Legal status |
| ||
| Pharmacokinetic data | |||
| Bioavailability | 80%+[4][5] | ||
| Protein binding | Weakly or not at all[4][5] | ||
| Metabolism | Liver (90%):[6][8] • Alcohol dehydrogenase • MEOS (CYP2E1) | ||
| Metabolites | Acetaldehyde; Acetic acid; Acetyl-CoA; Carbon dioxide; Ethyl glucuronide; Ethyl sulfate; Water | ||
| Onset of action | Peak concentrations:[6][4] • Range: 30–90 minutes • Mean: 45–60 minutes • Fasting: 30 minutes | ||
| Elimination half-life | Constant-rate elimination at typical concentrations:[7][8][6] • Range: 10–34 mg/dL/hour • Mean (men): 15 mg/dL/hour • Mean (women): 18 mg/dL/hr At very high concentrations (t1/2): 4.0–4.5 hours[5][4] | ||
| Duration of action | 6–16 hours (amount of time that levels are detectable)[9] | ||
| Excretion | • Major: metabolism (into carbon dioxide and water)[4] • Minor: urine, breath, sweat (5–10%)[6][4] | ||
| Identifiers | |||
| |||
| CAS Number |
| ||
| PubChem CID |
| ||
| IUPHAR/BPS |
| ||
| DrugBank |
| ||
| ChemSpider |
| ||
| UNII |
| ||
| KEGG |
| ||
| ChEBI |
| ||
| ChEMBL |
| ||
| PDB ligand |
| ||
| Chemical and physical data | |||
| Formula | C2H6O | ||
| Molar mass | 46.069 g·mol−1 | ||
| 3D model (JSmol) |
| ||
| Density | 0.7893 g/cm3 (at 20 °C)[10] | ||
| Melting point | −114.14 ± 0.03 °C (−173.45 ± 0.05 °F) [10] | ||
| Boiling point | 78.24 ± 0.09 °C (172.83 ± 0.16 °F) [10] | ||
| Solubility in water | Miscible mg/mL (20 °C) | ||
| |||
| |||


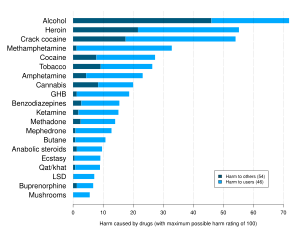
Ethanol is classified as a Group 1 carcinogen,[15] neurotoxin,[16][17] and birth defect agent.[18][19] The World Health Organization published a statement in The Lancet Public Health in April 2023 that "there is no safe amount that does not affect health".[20] A DrugScience 2010 study rated alcohol the most harmful drug overall, and the only drug more harmful to others than to the users themselves.[21]
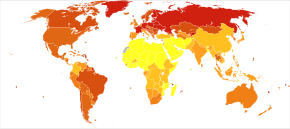
Alcohol serves various purposes, for example, it is one of the oldest and most commonly consumed recreational drugs, it is used for self-medication, and it is frequently involved in alcohol-related crimes such as drunk driving, public intoxication, and underage drinking. Some esoteric religions and schools incorporate the use of alcohol for spiritual purposes. However, alcohol has a variety of short-term and long-term adverse effects on health. Short-term effects from moderate consumption include happiness and euphoria, decreased anxiety, decreased social inhibition, sedation, impairment of cognitive, memory, motor, and sensory function, while binge drinking may result in generalized impairment of neurocognitive function, dizziness, analgesia, nausea, vomiting, hangover-like symptoms, blackout, and generalized depression of central nervous system (CNS) function. In high amounts, alcohol may cause alcohol intoxication characterized by loss of consciousness or, in severe cases, death; In 2016, 3.0 million deaths was responsible for excessive alcohol use worldwide.[22] Long-term effects are considered to be a major global public health issue[23] and includes alcoholism, abuse, withdrawal, fetal alcohol spectrum disorder (FASD), liver disease, hepatitis, cardiovascular disease such as cardiomyopathy, polyneuropathy, dementia, hallucinosis, brain damage, and cancers such as breast cancer. The adverse effects of alcohol on health are most important when it is used in excessive quantities or with heavy frequency. However, some of them, such as increased risk of certain cancers, may occur even with light or moderate alcohol consumption.[24][25][26]
Alcohol works in the brain primarily by increasing the effects of γ-Aminobutyric acid (GABA),[27] the major inhibitory neurotransmitter in the brain; by facilitating GABA's actions, alcohol suppresses the activity of the CNS.[27] The substance also directly affects a number of other neurotransmitter systems including those of glutamate, glycine, acetylcholine, and serotonin.[28][29] The pleasurable effects of alcohol ingestion are the result of increased levels of dopamine and endogenous opioids in the reward pathways of the brain.[30][31]
Uses edit
Dutch courage edit
Dutch courage, also known as pot-valiance or liquid courage, refers to courage gained from intoxication with alcohol.
Criminal edit
Albeit not a valid intoxication defense "liquid courage" is occasionally used as a tool to commit offenses such as drunk driving, thefts (for example motor vehicle thefts), alcohol-fueled robberies and violent crimes, or rape which sometimes but not always occurs in alcohol-facilitated sexual assaults where the victim is also drugged.
Consuming alcohol prior to visiting female sex workers is a common practice among some men.[32] Also, sex workers often resort to using drugs and alcohol to cope with stress. However, female sex workers in low- and middle-income countries have high rates of harmful alcohol use, which is associated with increased risk of risky sexual behavior.[33]
Warfare edit

The popular story dates the etymology of the term Dutch courage to English soldiers fighting in the Anglo-Dutch Wars[34] (1652–1674) and perhaps as early as the Thirty Years' War (1618–1648). One version states that jenever (or Dutch gin) was used by English soldiers for its calming effects before battle, and for its purported warming properties on the body in cold weather. Another version has it that English soldiers noted the bravery-inducing effects of jenever on Dutch soldiers.[35][36]
Alcohol has a long association of military use, and has been called "liquid courage" for its role in preparing troops for battle, anaesthetize injured soldiers, and celebrate military victories. It has also served as a coping mechanism for the intense stress of war and a means of decompression from combat to everyday life. However, this reliance on alcohol can have negative consequences for physical and mental health.[37] Military and veteran populations face significant challenges in addressing the co-occurrence of PTSD and alcohol use disorder.[38]
Food energy edit
The use of alcohol as a staple food source is considered inconvenient due to the fact that it increases the blood alcohol content (BAC). However, alcohol is a significant source of food energy for individuals with alcoholism and those who engage in binge drinking; For example, individuals with drunkorexia, engage in the combination of self-imposed malnutrition and binge drinking to avoid weight gain from alcohol, to save money for purchasing alcohol,[39] and to facilitate alcohol intoxication.[40]
The USDA uses a figure of 6.93 kilocalories (29.0 kJ) per gram of alcohol (5.47 kcal or 22.9 kJ per ml) for calculating food energy.[41] For distilled spirits, a standard serving in the United States is 44 ml (1.5 US fl oz), which at 40% ethanol (80 proof), would be 14 grams and 98 calories.
Alcoholic drinks are considered empty calorie foods because other than food energy they contribute no essential nutrients. According to the U.S. Department of Agriculture, based on NHANES 2013–2014 surveys, women in the US ages 20 and up consume on average 6.8 grams/day and men consume on average 15.5 grams/day.[42]
Alcohol is known to potentiate the insulin response of the human body to glucose, which, in essence, "instructs" the body to convert consumed carbohydrates into fat and to suppress carbohydrate and fat oxidation.[43][44] Ethanol is directly processed in the liver to acetyl CoA, the same intermediate product as in glucose metabolism. Because ethanol is mostly metabolized and consumed by the liver, chronic excessive use can lead to fatty liver. This leads to a chronic inflammation of the liver and eventually alcoholic liver disease.
Medical edit
When taken by mouth or injected into a vein ethanol is used to treat methanol or ethylene glycol toxicity[45] when fomepizole is not available.[46]
Ethanol, when used for toxicity, competes with other alcohols for the alcohol dehydrogenase enzyme, lessening metabolism into toxic aldehyde and carboxylic acid derivatives, and reducing more serious toxic effect of the glycols to crystallize in the kidneys.[47]
Recreational edit

Drinking culture is the set of traditions and social behaviors that surround the consumption of alcoholic beverages as a recreational drug and social lubricant. Although alcoholic beverages and social attitudes toward drinking vary around the world, nearly every civilization has independently discovered the processes of brewing beer, fermenting wine and distilling spirits.[48]
Common drinking styles include social drinking, binge drinking, drinking games, pub crawls, and sober curious.
Self-medication edit

The therapeutic index for ethanol is only 10%.[49]
Alcohol can have analgesic (pain-relieving) effects, which is why some people with chronic pain turn to alcohol to self-medicate and try to alleviate their physical discomfort.[50]
People with social anxiety disorder commonly self-medicate with alcohol to overcome their highly set inhibitions.[51] However, self-medicating excessively for prolonged periods of time with alcohol often makes the symptoms of anxiety or depression worse. This is believed to occur as a result of the changes in brain chemistry from long-term use.[52][53][54] A 2023 systematic review highlights the non-addictive use of alcohol for managing developmental issues, personality traits, and psychiatric symptoms, emphasizing the need for informed, harm-controlled approaches to alcohol consumption within a personalized health policy framework.[55]
Unscientific edit
In folk medicine, consuming a nightcap is for the purpose of inducing sleep. However, alcohol is not recommended by many doctors as a sleep aid because it interferes with sleep quality.[56]
"Hair of the dog", short for "hair of the dog that bit you", is a colloquial expression in the English language predominantly used to refer to alcohol that is consumed as a hangover remedy (with the aim of lessening the effects of a hangover). Many other languages have their own phrase to describe the same concept. The idea may have some basis in science in the difference between ethanol and methanol metabolism. Instead of alcohol, rehydration before going to bed or during hangover may relieve dehydration-associated symptoms such as thirst, dizziness, dry mouth, and headache.[57][58][59][60][61][62]
Drinking alcohol will not prevent or cure COVID-19,[63] contrary to some claims.[64] Instead, drinking alcohol may cause subclinical immunosuppression.[65]
Spiritual edit

Spiritual use of moderate alcohol consumption is found in some religions and schools with esoteric influences, including the Hindu tantra sect Aghori, in the Sufi Bektashi Order and Alevi Jem ceremonies,[66] in the Rarámuri religion, in the Japanese religion Shinto,[67] by the new religious movement Thelema, in Vajrayana Buddhism, and in Vodou faith of Haiti.
Contraindication edit

In the US, alcohol is subject to the FDA drug labeling Pregnancy Category X (Contraindicated in pregnancy).
Ethanol is classified as a teratogen[18][19][medical citation needed]—a substance known to cause birth defects; According to the U.S. Centers for Disease Control and Prevention (CDC), alcohol consumption by women who are not using birth control increases the risk of fetal alcohol syndrome. The CDC currently recommends complete abstinence from alcoholic beverages for women of child-bearing age who are pregnant, trying to become pregnant, or are sexually active and not using birth control.[68]
Minnesota, North Dakota, Oklahoma, South Dakota, and Wisconsin have laws that allow the state to involuntarily commit pregnant women to treatment if they abuse alcohol during pregnancy.[69]
Adverse effects edit

Alcohol has a variety of short-term and long-term adverse effects. Alcohol has both short-term, and long-term effects on the memory, and sleep. It also has reinforcement-related adverse effects, including addiction, dependence, and withdrawal. Alcohol use is directly related to considerable morbidity and mortality, for instance due to overdose and alcohol-related health problems.[70] The World Health Organization advises that there is no safe level of alcohol consumption.[71]
Drunkorexia is a colloquialism for anorexia or bulimia combined with an alcohol use disorder.[72]
Alcohol is a common cause of substance-induced psychosis or episodes, which may occur through acute intoxication, chronic alcoholism, withdrawal, exacerbation of existing disorders, or acute idiosyncratic reactions.[73] Research has shown that excessive alcohol use causes an 8-fold increased risk of psychotic disorders in men and a 3 fold increased risk of psychotic disorders in women.[74][75] While the vast majority of cases are acute and resolve fairly quickly upon treatment and/or abstinence, they can occasionally become chronic and persistent.[73] Alcoholic psychosis is sometimes misdiagnosed as another mental illness such as schizophrenia.[76]
An inability to process or exhibit emotions in a proper manner has been shown to exist in people who consume excessive amounts of alcohol and those who were exposed to alcohol while fetuses (FAexp).[77]
Short-term effects edit

The amount of ethanol in the body is typically quantified by blood alcohol content (BAC); weight of ethanol per unit volume of blood. Small doses of ethanol, in general, are stimulant-like[78] and produce euphoria and relaxation; people experiencing these symptoms tend to become talkative and less inhibited, and may exhibit poor judgement. At higher dosages (BAC > 1 gram/liter), ethanol acts as a central nervous system (CNS) depressant,[78] producing at progressively higher dosages, impaired sensory and motor function, slowed cognition, stupefaction, unconsciousness, and possible death. Ethanol is commonly consumed as a recreational substance, especially while socializing, due to its psychoactive effects.
Central nervous system impairment edit

Alcohol causes generalized CNS depression, is a positive allosteric GABAA modulator and is associated and related with cognitive, memory, motor, and sensory impairment. It slows and impairs cognition and reaction time and the cognitive skills, impairs judgement, interferes with motor function resulting in motor incoordination, loss of balance, confusion, sedation, numbness and slurred speech, impairs memory formation, and causes sensory impairment. At high concentrations, it can induce amnesia, analgesia, spins, stupor, and unconsciousness as result of high levels of ethanol in blood.
At very high concentrations, alcohol can cause anterograde amnesia, markedly decreased heart rate, pulmonary aspiration, positional alcohol nystagmus, respiratory depression, shock, coma and death can result due to profound suppression of CNS function alcohol overdose and can finish in consequent dysautonomia.
Gastrointestinal effects edit

Alcohol can cause nausea and vomiting in sufficiently high amounts (varying by person).
Alcohol stimulates gastric juice production, even when food is not present, and as a result, its consumption stimulates acidic secretions normally intended to digest protein molecules. Consequently, the excess acidity may harm the inner lining of the stomach. The stomach lining is normally protected by a mucosal layer that prevents the stomach from, essentially, digesting itself. However, in patients who have a peptic ulcer disease (PUD), this mucosal layer is broken down. PUD is commonly associated with the bacteria Helicobacter pylori, which secretes a toxin that weakens the mucosal wall, allowing acid and protein enzymes to penetrate the weakened barrier. Because alcohol stimulates the stomach to secrete acid, a person with PUD should avoid drinking alcohol on an empty stomach. Drinking alcohol causes more acid release, which further damages the already-weakened stomach wall.[79] Complications of this disease could include a burning pain in the abdomen, bloating and in severe cases, the presence of dark black stools indicate internal bleeding.[80] A person who drinks alcohol regularly is strongly advised to reduce their intake to prevent PUD aggravation.[80]
Ingestion of alcohol can initiate systemic pro-inflammatory changes through two intestinal routes: (1) altering intestinal microbiota composition (dysbiosis), which increases lipopolysaccharide (LPS) release, and (2) degrading intestinal mucosal barrier integrity – thus allowing LPS to enter the circulatory system. The major portion of the blood supply to the liver is provided by the portal vein. Therefore, while the liver is continuously fed nutrients from the intestine, it is also exposed to any bacteria and/or bacterial derivatives that breach the intestinal mucosal barrier. Consequently, LPS levels increase in the portal vein, liver and systemic circulation after alcohol intake. Immune cells in the liver respond to LPS with the production of reactive oxygen species, leukotrienes, chemokines and cytokines. These factors promote tissue inflammation and contribute to organ pathology.[81]
Holiday heart syndrome edit
Holiday heart syndrome, also known as alcohol-induced atrial arrhythmias, is a syndrome defined by an irregular heartbeat and palpitations[82] associated with high levels of ethanol consumption.[83][84] Holiday heart syndrome was discovered in 1978 when Philip Ettinger discovered the connection between arrhythmia and alcohol consumption.[85] It received its common name as it is associated with the binge drinking common during the holidays.[86] It is unclear how common this syndrome is. 5-10% of cases of atrial fibrillation may be related to this condition, but it could be as high 63%.[87]
Positional alcohol nystagmus edit
Positional alcohol nystagmus (PAN) is nystagmus (visible jerkiness in eye movement) produced when the head is placed in a sideways position. PAN occurs when the specific gravity of the membrane space of the semicircular canals in the ear differs from the specific gravity of the fluid in the canals because of the presence of alcohol.[88]
Specific population edit
Allergic-like reactions edit

Ethanol-containing beverages can cause alcohol flush reactions, exacerbations of rhinitis and, more seriously and commonly, bronchoconstriction in patients with a history of asthma, and in some cases, urticarial skin eruptions, and systemic dermatitis. Such reactions can occur within 1–60 minutes of ethanol ingestion, and may be caused by:[91]
- genetic abnormalities in the metabolism of ethanol, which can cause the ethanol metabolite, acetaldehyde, to accumulate in tissues and trigger the release of histamine, or
- true allergy reactions to allergens occurring naturally in, or contaminating, alcoholic beverages (particularly wine and beer), and
- other unknown causes.
Long-term effects edit
Due to the long term effects of alcohol abuse, binge drinking is considered to be a major public health issue.[23]
Prolonged heavy consumption of alcohol can cause significant permanent damage to the brain and other organs, resulting in dysfunction or death. The impact of alcohol on aging is multifaceted. The relationship between alcohol consumption and body weight is the subject of inconclusive studies. Alcoholic lung disease is disease of the lungs caused by excessive alcohol. However, the term 'alcoholic lung disease' is not a generally accepted medical diagnosis.
Alcoholism edit
Alcoholism or its medical diagnosis alcohol use disorder refers to alcohol addiction, alcohol dependence, dipsomania, and/or alcohol abuse. It is a major problem and many health problems as well as death can result from excessive alcohol use.[92][70] Alcohol dependence is linked to a lifespan that is reduced by about 12 years relative to the average person.[92] In 2004, it was estimated that 4% of deaths worldwide were attributable to alcohol use.[70] Deaths from alcohol are split about evenly between acute causes (e.g., overdose, accidents) and chronic conditions.[70] The leading chronic alcohol-related condition associated with death is alcoholic liver disease.[70] Alcohol dependence is also associated with cognitive impairment and organic brain damage.[92] Some researchers have found that even one alcoholic drink a day increases an individual's risk of health problems by 0.4%.[93]
Two or more consecutive alcohol-free days a week have been recommended to improve health and break dependence.[94][95]
Dry drunk is an expression coined by the founder of Alcoholics Anonymous [96] that describes an alcoholic who no longer drinks but otherwise maintains the same behavior patterns of an alcoholic.[97]
A high-functioning alcoholic (HFA) is a person who maintains jobs and relationships while exhibiting alcoholism.[98][99][100]
Many Native Americans in the United States have been harmed by, or become addicted to, drinking alcohol.[101]
Alcohol withdrawal syndrome edit

Discontinuation of alcohol after extended heavy use and associated tolerance development (resulting in dependence) can result in withdrawal. Alcohol withdrawal can cause confusion, paranoia, anxiety, insomnia, agitation, tremors, fever, nausea, vomiting, autonomic dysfunction, seizures, and hallucinations. In severe cases, death can result.
Delirium tremens is a condition that requires people with a long history of heavy drinking to undertake an alcohol detoxification regimen.
Alcohol is one of the more dangerous drugs to withdraw from.[103] Drugs which help to re-stabilize the glutamate system such as N-acetylcysteine have been proposed for the treatment of addiction to cocaine, nicotine, and alcohol.[104]
Alcoholic ketoacidosis edit
Alcoholic ketoacidosis (AKA) is a specific group of symptoms and metabolic state related to alcohol use.[105] Symptoms often include abdominal pain, vomiting, agitation, a fast respiratory rate, and a specific "fruity" smell.[106] Consciousness is generally normal.[107] Complications may include sudden death.[107]
Alcoholic polyneuropathy edit

Alcoholic polyneuropathy is a neurological disorder in which peripheral nerves throughout the body malfunction simultaneously. It is defined by axonal degeneration in neurons of both the sensory and motor systems and initially occurs at the distal ends of the longest axons in the body. This nerve damage causes an individual to experience pain and motor weakness, first in the feet and hands and then progressing centrally. Alcoholic polyneuropathy is caused primarily by chronic alcoholism; however, vitamin deficiencies are also known to contribute to its development.
edit
Alcohol-related dementia (ARD) is a form of dementia caused by long-term, excessive consumption of alcohol, resulting in neurological damage and impaired cognitive function.[108]
Alcohol and cardiovascular disease edit
Alcoholic cardiomyopathy edit

Alcoholic cardiomyopathy (ACM) is a disease in which the long-term consumption of alcohol leads to heart failure.[109] ACM is a type of dilated cardiomyopathy. The heart is unable to pump blood efficiently, leading to heart failure. It can affect other parts of the body if the heart failure is severe. It is most common in males between the ages of 35 and 50.
Austrian syndrome edit
Austrian syndrome, also known as Osler's triad, is a medical condition that was named after Robert Austrian in 1957. The presentation of the condition consists of pneumonia, endocarditis, and meningitis, all caused by Streptococcus pneumoniae. It is associated with alcoholism due to hyposplenism (reduced splenic functioning) and can be seen in males between the ages of 40 and 60 years old.[110] Robert Austrian was not the first one to describe the condition, but Richard Heschl (around 1860s) or William Osler were not able to link the signs to the bacteria because microbiology was not yet developed.
The leading cause of Osler's triad (Austrian syndrome) is Streptococcus pneumoniae, which is usually associated with heavy alcohol use.
Brain damage edit
Alcohol can cause brain damage,[111] Wernicke's encephalopathy and Alcoholic Korsakoff syndrome which frequently occur simultaneously, known as Wernicke–Korsakoff syndrome.[112] Lesions, or brain abnormalities, are typically located in the diencephalon which result in anterograde and retrograde amnesia, or memory loss.[112]
Cancer edit

The International Agency for Research on Cancer lists ethanol in alcoholic beverages as a Group 1 carcinogen in humans and argues that "There is sufficient evidence and research showing the carcinogenicity of acetaldehyde (the major metabolite of ethanol) which is excreted by the liver enzyme when one drinks alcohol."[15]
A 2001 meta-analysis did not find a clear safe level of alcohol consumption where there is no increased risk of cancer.[24] In 2020, alcohol was estimated to cause 750,000 cases of cancer worldwide, particularly esophagus, liver, and breast cancer.[113]
Cortisol edit
Research has looked into the effects of alcohol on the amount of cortisol that is produced in the human body. Continuous consumption of alcohol over an extended period of time has been shown to raise cortisol levels in the body. Cortisol is released during periods of high stress, and can result in the temporary shut down of other physical processes, causing physical damage to the body.
Liver damage edit

Consuming more than 30 grams of pure alcohol per day over an extended period can significantly increase the risk of developing alcoholic liver disease.[114] During the metabolism of alcohol via the respective dehydrogenases, nicotinamide adenine dinucleotide (NAD) is converted into reduced NAD. Normally, NAD is used to metabolize fats in the liver, and as such alcohol competes with these fats for the use of NAD. Prolonged exposure to alcohol means that fats accumulate in the liver, leading to the term 'fatty liver'. Continued consumption (such as in alcohol use disorder) then leads to cell death in the hepatocytes as the fat stores reduce the function of the cell to the point of death. These cells are then replaced with scar tissue, leading to the condition called cirrhosis.
Specific population edit
- Pregnant women: Babies exposed to alcohol, benzodiazepines, barbiturates, and some antidepressants (SSRIs) during pregnancy may experience neonatal withdrawal.[115]
Other effects edit
Frequent drinking of alcoholic beverages is a major contributing factor in cases of elevated blood levels of triglycerides.[116]
Social issues edit

Alcohol causes a plethora of detrimental effects in society.[92] Many emergency room visits involve alcohol use.[92] As many as 15% of employees show problematic alcohol-related behaviors in the workplace, such as drinking before going to work or even drinking on the job.[92]
Individuals who engage with or share alcohol-related content on social networking services tend to exhibit higher levels of alcohol use and related issues.[118] Alcohol availability and consumption rates and alcohol rates are positively associated with nuisance, loitering, panhandling, and disorderly conduct in public space.[119] Recent research indicates that the abundance of alcohol retailers and the availability of inexpensive alcoholic beverages are linked to heavy alcohol consumption among college students.[120] Also, joblessness can heighten the risk of alcohol consumption and smoking.[121]
edit

Alcohol use is stereotypically associated with crime,[119] both violent and non-violent.[92] Some crimes are uniquely tied to alcohol, such as public intoxication or underage drinking, while others are simply more likely to occur together with alcohol consumption. Crime perpetrators are much more likely to be intoxicated than crime victims. Many alcohol laws have been passed to criminalize various alcohol-related activities.[119][122] Underage drinking and drunk driving are the most prevalent alcohol‐specific offenses in the United States[119] and a major problem in many countries worldwide.[123][124][125] About one-third of arrests in the United States involve alcohol misuse,[92] and arrests for alcohol-related crimes constitute a high proportion of all arrests made by police in the U.S. and elsewhere.[126] In general, programs aimed at reducing society's consumption of alcohol, including education in schools, are seen as an effective long-term solution. Strategies aiming to reduce alcohol consumption among adult offenders have various estimates of effectiveness.[127] Policing alcohol‐related street disorder and enforcing compliance checks of alcohol‐dispensing businesses has proven successful in reducing public perception of and fear of criminal activities.[119]
In the early 2000s, the monetary cost of alcohol-related crime in the United States alone has been estimated at over $205 billion, twice the economic cost of all other drug-related crimes.[128] In a similar period in the United Kingdom, the cost of crime and its antisocial effects was estimated at £7.3 billion.[127] Another estimate for the UK for yearly cost of alcohol-related crime suggested double that estimate, at between £8 and 13 billion.[129] Risky patterns of drinking are particularly problematic in and around Russia, Mexico and some parts of Africa.[130] Alcohol is more commonly associated with both violent and non-violent crime than are drugs like marijuana.[92]
Passive drinking, like passive smoking, refers to the damage done to others as a result of drinking alcoholic beverages. These include the unborn fetus and children of parents who drink excessively, drunk drivers, accidents, domestic violence and alcohol-related sexual assaults[131]
Automobile accidents edit

A 2002 study found 41% of people fatally injured in traffic accidents were in alcohol-related crashes.[132] Misuse of alcohol is associated with more than 40% of deaths that occur in automobile accidents every year.[92] The risk of a fatal car accident increases exponentially with the level of alcohol in the driver's blood.[133]
Most countries have passed laws prohibiting driving a motor vehicle while impaired by alcohol. In the U.S., these crimes are generally referred to as driving under the influence (DUI), although there are many naming variations among jurisdictions, such as driving while intoxicated (DWI).[134] With alcohol consumption, a drunk driver's level of intoxication is typically determined by a measurement of blood alcohol content or BAC; but this can also be expressed as a breath test measurement, often referred to as a BrAC. A BAC or BrAC measurement in excess of the specific threshold level, such as 0.08% in the U.S.,[135] defines the criminal offense with no need to prove impairment.[136] In some jurisdictions, there is an aggravated category of the offense at a higher BAC level, such as 0.12%, 0.15% or 0.25%. In many jurisdictions, police officers can conduct field tests of suspects to look for signs of intoxication.
Methanol laced alcohol edit

Outbreaks of methanol poisoning have occurred when methanol is used to lace moonshine (bootleg liquor).[137] This is commonly done to bulk up the original product to gain profit. Because of its similarities in both appearance and odor to ethanol (the alcohol in beverages), it is difficult to differentiate between the two.
Methanol is a toxic alcohol. If as little as 10 mL of pure methanol is ingested, for example, it can break down into formic acid, which can cause permanent blindness by destruction of the optic nerve, and 30 mL is potentially fatal,[138] although the median lethal dose is typically 100 mL (3.4 fl oz) (i.e. 1–2 mL/kg body weight of pure methanol[139]). Reference dose for methanol is 2.0 mg/kg/day.[140] Toxic effects take hours to start, and effective antidotes can often prevent permanent damage.[138]
India has a thriving moonshine industry, and methanol-tainted batches have killed over 2,000 people in the last 3 decades.
Public drunkenness edit

Public drunkenness or intoxication is a common problem in many jurisdictions. Public intoxication laws vary widely by jurisdiction, but include public nuisance laws, open-container laws, and prohibitions on drinking alcohol in public or certain areas. The offenders are often lower class individuals and this crime has a very high recidivism rate, with numerous instances of repeated instances of the arrest, jail, release without treatment cycle. The high number of arrests for public drunkenness often reflects rearrests of the same offenders.[126]
Sexual assault edit

Often, a victim becomes incapacitated due to having consumed alcohol, which then facilitates sexual assault or rape, a crime known as drug-facilitated sexual assault (DFSA).[143][144] Alcohol remains the most commonly used predator drug,[145][146] and is said to be used in the majority of sexual assaults.[147] Over 50% of reported rapes involve alcohol.[clarification needed][92] Many assailants use alcohol because their victims often willingly imbibe it, and can be encouraged to drink enough to lose inhibitions or consciousness. Sex with an unconscious victim is considered rape in most if not all jurisdictions, and some assailants have committed "rapes of convenience" whereby they have assaulted a victim after he or she had become unconscious from drinking too much.[148]
Caffeinated alcoholic drinks are particularly implicated in DFSA.[149][150]
Alcohol abuse increases the risk of individuals either experiencing or perpetrating sexual violence and risky, casual sex.[151]
Violent crime edit

The World Health Organization has noted that out of social problems created by the harmful use of alcohol, "crime and violence related to alcohol consumption" are likely the most significant issue.[130] In the United States, 15% of robberies, 63% of intimate partner violence incidents, 37% of sexual assaults, 45–46% of physical assaults and 40–45% of homicides (murders) involved use of alcohol.[153][128] A 1983 study for the United States found that 54% of violent crime perpetrators, arrested in that country, had been consuming alcohol before their offenses.[126] In 2002, it was estimated that 1 million violent crimes in the U.S. were related to alcohol use.[92] More than 43% of violent encounters with police involve alcohol.[92] Alcohol is implicated in more than two-thirds of cases of intimate partner violence.[92] Studies also suggest there may be links between alcohol abuse and child abuse.[119] In the United Kingdom, in 2015/2016, 39% of those involved in violent crimes were under alcohol influence.[154] International studies are similar, with an estimate that 63% of violent crimes worldwide involves the use of alcohol.[128]
The relation between alcohol and violence is not yet fully understood, as its impact on different individuals varies.[citation needed] Studies and theories of alcohol abuse suggest, among others, that use of alcohol likely reduces the offender's perception and awareness of consequences of their actions.[147][119][126][155] Heavy drinking is associated with vulnerability to injury, marital discord, and domestic violence.[92] Moderate drinkers are more frequently engaged in intimate violence than are light drinkers and abstainers, however generally it is heavy and/or binge drinkers who are involved in the most chronic and serious forms of aggression. Research found that factors that increase the likelihood of alcohol‐related violence include difficult temperament, hyperactivity, hostile beliefs, history of family violence, poor school performance, delinquent peers, criminogenic beliefs about alcohol's effects, impulsivity, and antisocial personality disorder. The odds, frequency, and severity of physical attacks are all positively correlated with alcohol use. In turn, violence decreases after behavioral marital alcoholism treatment.[119]
Binge drinking edit

Binge drinking is a style of drinking that is popular in several countries worldwide, and overlaps somewhat with social drinking since it is often done in groups. The degree of intoxication however, varies between and within various cultures that engage in this practice. A binge on alcohol can occur over hours, last up to several days, or in the event of extended abuse, even weeks. Due to the long term effects of alcohol abuse, binge drinking is considered to be a major public health issue.[23]
Binge drinking is more common in males, during adolescence and young adulthood. Heavy regular binge drinking is associated with adverse effects on neurologic, cardiac, gastrointestinal, hematologic, immune, and musculoskeletal organ systems as well as increasing the risk of alcohol induced psychiatric disorders.[156][157] A US-based review of the literature found that up to one-third of adolescents binge-drink, with 6% reaching the threshold of having an alcohol-related substance use disorder.[158] Approximately one in 25 women binge-drinks during pregnancy, which can lead to fetal alcohol syndrome and fetal alcohol spectrum disorders.[159] Binge drinking during adolescence is associated with traffic accidents and other types of accidents, violent behavior as well as suicide. The more often a child or adolescent binge drinks and the younger they are the more likely that they will develop an alcohol use disorder including alcoholism. A large number of adolescents who binge-drink also consume other psychotropic substances.[160]
Environment edit

Alcoholic beverage containers, particularly broken glass bottles, are a common source of litter that is difficult to clean up, which may puncture bicycle tires, hurt wild life animals, etc. Alcoholic bottles are often discarded improperly, not recycled, or left in public spaces, which have negative impacts on the environment. Alcohol may negatively impact decision making in taking environmental responsibility.
Hurtful communication edit

Alcohol may cause hurtful communication.
Drunk dialing edit
Drunk dialing refers to an intoxicated person making phone calls that they would not likely make if sober, often a lonely individual calling former or current love interests.
A 2021 study, that examined the relationship between drunk texting and emotional dysregulation, found a positive correlation. The findings suggest that interventions targeting emotional regulation skills may be beneficial.[161]
In vino veritas edit
In vino veritas is a Latin phrase that means 'in wine, there is truth', suggesting a person under the influence of alcohol is more likely to speak their hidden thoughts and desires.
Suicide edit
Most people are under the influence of sedative-hypnotic drugs (such as alcohol or benzodiazepines) when they die by suicide,[162] with alcoholism present in between 15% and 61% of cases.[163] Countries that have higher rates of alcohol use and a greater density of bars generally also have higher rates of suicide.[164] About 2.2–3.4% of those who have been treated for alcoholism at some point in their life die by suicide.[164] Alcoholics who attempt suicide are usually male, older, and have tried to take their own lives in the past.[163] In adolescents who misuse alcohol, neurological and psychological dysfunctions may contribute to the increased risk of suicide.[165]
Overdose edit

Symptoms of ethanol overdose may include nausea, vomiting, CNS depression, coma, acute respiratory failure, or death. Levels of even less than 0.1% can cause intoxication, with unconsciousness often occurring at 0.3–0.4%.[166] Death from ethanol consumption is possible when blood alcohol levels reach 0.4%. A blood level of 0.5% or more is commonly fatal. The oral median lethal dose (LD50) of ethanol in rats is 5,628 mg/kg. Directly translated to human beings, this would mean that if a person who weighs 70 kg (150 lb) drank a 500 mL (17 US fl oz) glass of pure ethanol, they would theoretically have a 50% risk of dying. The highest blood alcohol level ever recorded, in which the subject survived, is 1.41%.[167]
Interactions edit
Disorders edit
Diabetes edit
See the insulin section.
Heptatitis edit
Alcohol consumption can be especially dangerous for those with pre-existing liver damage from hepatitis B or C. Even relatively low amounts of alcohol can be life-threatening in these cases,[22] so a strict adherence to abstinence is highly recommended.[168]
Hitamine intolerance edit
Alcohol may release histamine in individuals with histamine intolerance.[169]
Dosage forms edit
Alcohol induced dose dumping (AIDD) edit
This dose dumping effect is an unintended rapid release of large amounts of a given drug, when administered through a modified-release dosage while co-ingesting ethanol.[170] This is considered a pharmaceutical disadvantage due to the high risk of causing drug-induced toxicity by increasing the absorption and serum concentration above the therapeutic window of the drug. The best way to prevent this interaction is by avoiding the co-ingestion of both substances or using specific controlled-release formulations that are resistant to AIDD.
Drugs edit
Alcohol can intensify the sedation caused by antipsychotics, and certain antidepressants.[166]
Alcohol combined with cannabis (not to be confused with tincture of cannabis which contains minute quantities of alcohol) — known as cross-fading and may easily cause spins in people who are drunk and smoke potent cannabis; Ethanol increases plasma tetrahydrocannabinol levels, which suggests that ethanol may increase the absorption of tetrahydrocannabinol.[171]
TOMSO is a lesser-known psychedelic drug and a substituted amphetamine. TOMSO is inactive on its own; it is activated with the consumption of alcohol.
Hypnotics/sedatives edit

Alcohol can intensify the sedation caused by hypnotics/sedatives such as barbiturates, benzodiazepines, sedative antihistamines, opioids, nonbenzodiazepines/Z-drugs (such as zolpidem and zopiclone).[166]
Disulfiram-like drugs edit
Disulfiram edit
Disulfiram inhibits the enzyme acetaldehyde dehydrogenase, which in turn results in buildup of acetaldehyde, a toxic metabolite of ethanol with unpleasant effects. The medication or drug is commonly used to treat alcohol use disorder, and results in immediate hangover-like symptoms upon consumption of alcohol, this effect is widely known as disulfiram effect.
Metronidazole edit
Metronidazole is an antibacterial agent that kills bacteria by damaging cellular DNA and hence cellular function.[172] Metronidazole is usually given to people who have diarrhea caused by Clostridium difficile bacteria. Patients who are taking metronidazole are sometimes advised to avoid alcohol, even after 1 hour following the last dose. Although older data suggested a possible disulfiram-like effect of metronidazole, newer data has challenged this and suggests it does not actually have this effect.
Insulin edit
Alcohol consumption can cause hypoglycemia in diabetics on certain medications, such as insulin or sulfonylurea, by blocking gluconeogenesis.[173]
NSAIDs edit
The concomitant use of NSAIDs with alcohol and/or tobacco products significantly increases the already elevated risk of peptic ulcers during NSAID therapy.[174][better source needed]
Stimulants edit

Ethanol interacts with cocaine in vivo to produce cocaethylene, another psychoactive substance which may be substantially more cardiotoxic than either cocaine or alcohol by themselves.[175][176]
Ethylphenidate formation appears to be more common when large quantities of methylphenidate and alcohol are consumed at the same time, such as in non-medical use or overdose scenarios.[177] However, only a small percent of the consumed methylphenidate is converted to ethylphenidate.[178]
A nicotini is any alcoholic drink which includes nicotine as an ingredient. Its name is modeled after the word "martini" in the fashion of such drinks as the appletini. Tobacco and nicotine increase alcohol craving.[179]
Methanol and ethylene glycol edit
The rate-limiting steps for the elimination of ethanol are in common with certain other substances. As a result, the blood alcohol concentration can be used to modify the rate of metabolism of toxic alcohols, such as methanol and ethylene glycol. Methanol itself is not highly toxic, but its metabolites formaldehyde and formic acid are; therefore, to reduce the rate of production and concentration of these harmful metabolites, ethanol can be ingested.[180] Ethylene glycol poisoning can be treated in the same way.
Warfarin edit
Excessive use of alcohol is also known to affect the metabolism of warfarin and can elevate the INR, and thus increase the risk of bleeding.[181] The U.S. Food and Drug Administration (FDA) product insert on warfarin states that alcohol should be avoided.[182] The Cleveland Clinic suggests that when taking warfarin one should not drink more than "one beer, 6 oz of wine, or one shot of alcohol per day".[183]
Special population edit
Isoniazid edit
Levels of liver enzymes in the bloodstream should be frequently checked in daily alcohol drinkers, pregnant women, IV drug users, people over 35, and those who have chronic liver disease, severe kidney dysfunction, peripheral neuropathy, or HIV infection since they are more likely to develop hepatitis from INH.[184][185]
Pharmacology edit
Pharmacodynamics edit

The principal mechanism of action for ethanol has proven elusive and remains not fully understood.[27][186] Identifying molecular targets for ethanol has proven unusually difficult, in large part due to its unique biochemical properties.[186] Specifically, ethanol is a very low molecular weight compound and is of exceptionally low potency in its actions, causing effects only at very high (millimolar mM) concentrations.[186][187] For these reasons, unlike with most drugs, it has not yet been possible to employ traditional biochemical techniques to directly assess the binding of ethanol to receptors or ion channels.[186][187] Instead, researchers have had to rely on functional studies to elucidate the actions of ethanol.[186] Moreover, although it has been established that ethanol modulates ion channels to mediate its effects,[29] ion channels are complex proteins, and their interactions and functions are complicated by diverse subunit compositions and regulation by conserved cellular signals (e.g. signaling lipids).[27][186]
Much progress has been made in understanding the pharmacodynamics of ethanol over the last few decades.[28][186] While no binding sites have been identified and established unambiguously for ethanol at present, it appears that it affects ion channels, in particular ligand-gated ion channels, to mediate its effects in the CNS.[27][28][29][186] Ethanol has specifically been found in functional assays to enhance or inhibit the activity of a variety of ion channels, including the GABAA receptor, the ionotropic glutamate AMPA, kainate, and NMDA receptors, the glycine receptor,[188] the nicotinic acetylcholine receptors,[189] the serotonin 5-HT3 receptor, voltage-gated calcium channels, and BK channels, among others.[27][28][29][190][191] However, many of these actions have been found to occur only at very high concentrations that may not be pharmacologically significant at recreational doses of ethanol, and it is unclear how or to what extent each of the individual actions is involved in the effects of ethanol.[186] In any case, ethanol has long shown a similarity in its effects to positive allosteric modulators of the GABAA receptor like benzodiazepines, barbiturates, and various general anesthetics.[27][186] Indeed, ethanol has been found to enhance GABAA receptor-mediated currents in functional assays.[27][186] In accordance, it is theorized and widely believed that the primary mechanism of action is as a GABAA receptor positive allosteric modulator.[27][186] However, the diverse actions of ethanol on other ion channels may be and indeed likely are involved in its effects as well.[28][186]
In 2007, it was discovered that ethanol potentiates extrasynaptic δ subunit-containing GABAA receptors at behaviorally relevant (as low as 3 mM) concentrations.[27][186][192] This is in contrast to previous functional assays of ethanol on γ subunit-containing GABAA receptors, which it enhances only at far higher concentrations (> 100 mM) that are in excess of recreational concentrations (up to 50 mM).[27][186][193] Ro15-4513, a close analogue of the benzodiazepine antagonist flumazenil (Ro15-1788), has been found to bind to the same site as ethanol and to competitively displace it in a saturable manner.[186][192] In addition, Ro15-4513 blocked the enhancement of δ subunit-containing GABAA receptor currents by ethanol in vitro.[186] In accordance, the drug has been found to reverse many of the behavioral effects of low-to-moderate doses of ethanol in rodents, including its effects on anxiety, memory, motor behavior, and self-administration.[186][192] Taken together, these findings suggest a binding site for ethanol on subpopulations of the GABAA receptor with specific subunit compositions via which it interacts with and potentiates the receptor.[27][186][192][194]
A 2019 study showed the accumulation of an unnatural lipid phosphatidylethanol (PEth) competes with PIP2 agonist sites on lipid-gated ion channels.[195] This presents a novel indirect mechanism and suggests that a metabolite, not the ethanol itself, can affect the primary targets of ethanol intoxication. Many of the primary targets of ethanol are known to bind PIP2 including GABAA receptors,[196] but the role of PEth will need to be investigated for each of the primary targets.
Rewarding and reinforcing actions edit

The reinforcing effects of alcohol consumption are mediated by acetaldehyde generated by catalase and other oxidizing enzymes such as cytochrome P-4502E1 in the brain.[199] Although acetaldehyde has been associated with some of the adverse and toxic effects of ethanol, it appears to play a central role in the activation of the mesolimbic dopamine system.[200]
Ethanol's rewarding and reinforcing (i.e., addictive) properties are mediated through its effects on dopamine neurons in the mesolimbic reward pathway, which connects the ventral tegmental area to the nucleus accumbens (NAcc).[201][202] One of ethanol's primary effects is the allosteric inhibition of NMDA receptors and facilitation of GABAA receptors (e.g., enhanced GABAA receptor-mediated chloride flux through allosteric regulation of the receptor).[203] At high doses, ethanol inhibits most ligand-gated ion channels and voltage-gated ion channels in neurons as well.[203]
With acute alcohol consumption, dopamine is released in the synapses of the mesolimbic pathway, in turn heightening activation of postsynaptic D1 receptors.[201][202] The activation of these receptors triggers postsynaptic internal signaling events through protein kinase A, which ultimately phosphorylate cAMP response element binding protein (CREB), inducing CREB-mediated changes in gene expression.[201][202]
With chronic alcohol intake, consumption of ethanol similarly induces CREB phosphorylation through the D1 receptor pathway, but it also alters NMDA receptor function through phosphorylation mechanisms;[201][202] an adaptive downregulation of the D1 receptor pathway and CREB function occurs as well.[201][202] Chronic consumption is also associated with an effect on CREB phosphorylation and function via postsynaptic NMDA receptor signaling cascades through a MAPK/ERK pathway and CAMK-mediated pathway.[202] These modifications to CREB function in the mesolimbic pathway induce expression (i.e., increase gene expression) of ΔFosB in the NAcc,[202] where ΔFosB is the "master control protein" that, when overexpressed in the NAcc, is necessary and sufficient for the development and maintenance of an addictive state (i.e., its overexpression in the nucleus accumbens produces and then directly modulates compulsive alcohol consumption).[202][204][205][206]
Relationship between concentrations and effects edit
| mg/dL | mM | % v/v | Effects |
|---|---|---|---|
| 50 | 11 | 0.05% | Euphoria, talkativeness, relaxation, happiness, gladness, pleasure, joyfulness. |
| 100 | 22 | 0.1% | Central nervous system depression, anxiety suppression, stress suppression, sedation, nausea, possible vomiting. Impaired motor, memory, cognition and sensory function. |
| >140 | 30 | >0.14% | Decreased blood flow to brain, slurred speech, double or blurry vision. |
| 300 | 65 | 0.3% | Stupefaction, confusion, numbness, dizziness, loss of consciousness. |
| 400 | 87 | 0.4% | Ethylic intoxication, drunkenness, inebriation, alcohol poisoning or possible death. |
| 500 | 109 | >0.55% | Unconsciousness, coma and death. |
Recreational concentrations of ethanol are typically in the range of 1 to 50 mM.[193][27] Very low concentrations of 1 to 2 mM ethanol produce zero or undetectable effects except in alcohol-naive individuals.[193] Slightly higher levels of 5 to 10 mM, which are associated with light social drinking, produce measurable effects including changes in visual acuity, decreased anxiety, and modest behavioral disinhibition.[193] Further higher levels of 15 to 20 mM result in a degree of sedation and motor incoordination that is contraindicated with the operation of motor vehicles.[193] In jurisdictions in the U.S., maximum blood alcohol levels for legal driving are about 17 to 22 mM.[208][209] In the upper range of recreational ethanol concentrations of 20 to 50 mM, depression of the central nervous system is more marked, with effects including complete drunkenness, profound sedation, amnesia, emesis, hypnosis, and eventually unconsciousness.[193][208] Levels of ethanol above 50 mM are not typically experienced by normal individuals and hence are not usually physiologically relevant; however, such levels – ranging from 50 to 100 mM – may be experienced by alcoholics with high tolerance to ethanol.[193] Concentrations above this range, specifically in the range of 100 to 200 mM, would cause death in all people except alcoholics.[193]
List of known actions in the central nervous system edit
Ethanol has been reported to possess the following actions in functional assays at varying concentrations:[187]
- GABAA receptor positive allosteric modulator (primarily of δ subunit-containing receptors)[203]
- NMDA receptor negative allosteric modulator[191][203]
- Decreased levels of nitric oxide in brain medulla[210]
- Increased levels of dopamine and endogenous opioids in the mesolimbic pathway, secondary to other actions[200][203]
- AMPA receptor negative allosteric modulator[191]
- Kainate receptor negative allosteric modulator[191]
- Glycine receptor positive allosteric modulator[188]
- Serotonin receptor positive allosteric modulator[188]
- Opioid receptor endogenous positive allosteric modulator[191]
- Muscarinic acetylcholine receptor positive allosteric modulator.
- Nicotinic acetylcholine receptor positive allosteric modulator[189][211]
- 5-HT3 receptor positive allosteric modulator
- Glycine reuptake inhibitor[212]
- Adenosine reuptake inhibitor[213]
- L-type calcium channel blocker
- GIRK channel opener
Some of the actions of ethanol on ligand-gated ion channels, specifically the nicotinic acetylcholine receptors and the glycine receptor, are dose-dependent, with potentiation or inhibition occurring dependent on ethanol concentration.[187] This seems to be because the effects of ethanol on these channels are a summation of positive and negative allosteric modulatory actions.[187]
Pharmacokinetics edit
Absorption edit
Ethanol can be administered orally, by inhalation, rectally, or by injection (e.g., intravenous),[6][214] though it is typically ingested simply via oral administration.[4] The oral bioavailability of ethanol is around 80% or more.[4][5] In fasting volunteers, blood levels of ethanol increase proportionally with the dose of ethanol administered.[214] Blood alcohol concentrations may be estimated by dividing the amount of ethanol ingested by the body weight of the individual and correcting for water dilution.[6]
Onset edit

Peak circulating levels of ethanol are usually reached within a range of 30 to 90 minutes of ingestion, with an average of 45 to 60 minutes.[6][4] People who have fasted overnight have been found to reach peak ethanol concentrations more rapidly, at within 30 minutes of ingestion.[6]
The onset varies depends on the type of alcoholic drink:[215]
- Vodka tonic: 36 ± 10 minutes
- Wine: 54 ± 14 minutes
- Beer: 62 ± 23 minutes
Also, carbonated alcoholic drinks seem to have a shorter onset compare to flat drinks in the same volume. One theory is that carbon dioxide in the bubbles somehow speeds the flow of alcohol into the intestines.[216]
Food in the gastrointestinal system and hence gastric emptying is the most important factor that influences the absorption of orally ingested ethanol.[6][214] The absorption of ethanol is much more rapid on an empty stomach than with a full one.[6] The delay in ethanol absorption caused by food is similar regardless of whether food is consumed just before, at the same time, or just after ingestion of ethanol.[6] The type of food, whether fat, carbohydrates, or protein, also is of little importance.[214] Not only does food slow the absorption of ethanol, but it also reduces the bioavailability of ethanol, resulting in lower circulating concentrations.[6]
Distribution edit
Upon ingestion, ethanol is rapidly distributed throughout the body.[4] It is distributed most rapidly to tissues with the greatest blood supply.[6] As such, ethanol primarily affects the brain, liver, and kidneys.[4] Other tissues with lower circulation, such as bone, require more time for ethanol to distribute into.[6] Ethanol crosses biological membranes and the blood–brain barrier easily, through a simple process of passive diffusion.[4][214] The volume of distribution of ethanol is around .55 L/kg (0.53 US pt/lb).[4] It is only weakly or not at all plasma protein bound.[4][5]
Metabolism edit

Approximately 90% of the metabolism of ethanol occurs in the liver.[6][8] This occurs predominantly via the enzyme alcohol dehydrogenase, which transforms ethanol into its metabolite acetaldehyde (ethanal).[6][8] Acetaldehyde is subsequently metabolized by the enzyme aldehyde dehydrogenase into acetate (ethanoate), which in turn is broken down into carbon dioxide and water.[6] Acetate also combines with coenzyme A to form acetyl-CoA, and hence may participate in metabolic pathways.[4] Alcohol dehydrogenase and aldehyde dehydrogenase are present at their highest concentrations in the liver, but are widely expressed throughout the body, and alcohol dehydrogenase may also be present in the stomach and small intestine.[4] Aside from alcohol dehydrogenase, the microsomal ethanol-oxidizing system (MEOS), specifically mediated by the cytochrome P450 enzyme CYP2E1, is the other major route of ethanol metabolism.[6][8] CYP2E1 is inducible by ethanol, so while alcohol dehydrogenase handles acute or low concentrations of ethanol, MEOS is predominant with higher concentrations or with repeated/chronic use.[6][8] A small amount of ethanol undergoes conjugation to form ethyl glucuronide and ethyl sulfate.[4] There may also be another metabolic pathway that metabolizes as much as 25 to 35% of ethanol at typical concentrations.[5]
At even low physiological concentrations, ethanol completely saturates alcohol dehydrogenase.[6] This is because ethanol has high affinity for the enzyme and very high concentrations of ethanol occur when it is used as a recreational substance.[6] For this reason, the metabolism of ethanol follows zero-order kinetics at typical physiological concentrations.[8] That is, ethanol does not have an elimination half-life (i.e., is not metabolized at an exponential rate), and instead, is eliminated from the circulation at a constant rate.[8][7] The mean elimination rates for ethanol are 15 mg/dL per hour for men and 18 mg/dL per hour for women, with a range of 10 to 34 mg/dL per hour.[8][6] At very high concentrations, such as in overdose, it has been found that the rate of elimination of ethanol is increased.[5] In addition, ethanol metabolism follows first-order kinetics at very high concentrations, with an elimination half-life of about 4 or 4.5 hours (which implies a clearance rate of approximately 6 L/hour/70 kg).[5][4] This seems to be because other processes, such as the MEOS/CYP2E1, also become involved in the metabolism of ethanol at higher concentrations.[4] However, the MEOS/CYP2E1 alone does not appear sufficient to fully explain the increase in ethanol metabolism rate.[5]
Some individuals have less effective forms of one or both of the metabolizing enzymes of ethanol, and can experience more marked symptoms from ethanol consumption than others.[217] However, those having acquired alcohol tolerance have a greater quantity of these enzymes, and metabolize ethanol more rapidly.[217]
Elimination edit
Ethanol is mainly eliminated from the body via metabolism into carbon dioxide and water.[6] Around 5 to 10% of ethanol that is ingested is eliminated unchanged in urine, breath, and sweat.[4] Transdermal alcohol that diffuses through the skin as insensible perspiration or is exuded as sweat (sensible perspiration) can be detected using wearable sensor technology[218] such as SCRAM ankle bracelet[219] or the more discreet ION Wearable.[220] Ethanol or its metabolites may be detectable in urine for up to 96 hours (3–5 days) after ingestion.[4]
Chemistry edit
Ethanol is also known chemically as alcohol, ethyl alcohol, or drinking alcohol. It is a simple alcohol with a molecular formula of C2H6O and a molecular weight of 46.0684 g/mol. The molecular formula of ethanol may also be written as CH3−CH2−OH or as C2H5−OH. The latter can also be thought of as an ethyl group linked to a hydroxyl (alcohol) group and can be abbreviated as EtOH. Ethanol is a volatile, flammable, colorless liquid with a slight characteristic odor. Aside from its use as a psychoactive and recreational substance, ethanol is also commonly used as an antiseptic and disinfectant, a chemical and medicinal solvent, and a fuel.
Production edit
Ethanol is produced naturally as a byproduct of the metabolic processes of yeast and hence is present in any yeast habitat, including even endogenously in humans, but it does not cause raised blood alcohol content as seen in the rare medical condition auto-brewery syndrome (ABS). It is manufactured through hydration of ethylene or by brewing via fermentation of sugars with yeast (most commonly Saccharomyces cerevisiae). The sugars are commonly obtained from sources like steeped cereal grains (e.g., barley), grape juice, and sugarcane products (e.g., molasses, sugarcane juice). Ethanol–water mixture which can be further purified via distillation.
Home-made alcoholic beverages edit
Homebrewing edit

Homebrewing is the brewing of beer or other alcoholic beverages on a small scale for personal, non-commercial purposes. Supplies, such as kits and fermentation tanks, can be purchased locally at specialty stores or online. Beer was brewed domestically for thousands of years before its commercial production, although its legality has varied according to local regulation. Homebrewing is closely related to the hobby of home distillation, the production of alcoholic spirits for personal consumption; however home distillation is generally more tightly regulated.
Moonshine edit
Although methanol is not produced in toxic amounts by fermentation of sugars from grain starches,[221] it is a major occurrence in fruit spirits.[222] However, in modern times, reducing methanol with the absorption of a molecular sieve is a practical method for production.[223]
Analogues edit

Ethanol has a variety of analogues, many of which have similar actions and effects. Methanol (methyl alcohol) and isopropyl alcohol (also called rubbing alcohol) are toxic alcohols, and thus unsafe for human consumption.[11] Methanol is the most toxic alcohol; the toxicity of isopropyl alcohol lies between that of ethanol and methanol, and is about twice that of ethanol.[224] In general, higher alcohols are less toxic.[224] n-Butanol is reported to produce similar effects to those of ethanol and relatively low toxicity (one-sixth of that of ethanol in one rat study).[225][226] However, its vapors can produce eye irritation and inhalation can cause pulmonary edema.[224] Acetone (propanone) is a ketone rather than an alcohol, and is reported to produce similar toxic effects; it can be extremely damaging to the cornea.[224]
The tertiary alcohol tert-amyl alcohol (TAA), also known as 2-methylbutan-2-ol (2M2B), has a history of use as a hypnotic and anesthetic, as do other tertiary alcohols such as methylpentynol, ethchlorvynol, and chloralodol. Unlike primary alcohols like ethanol, these tertiary alcohols cannot be oxidized into aldehyde or carboxylic acid metabolites, which are often toxic, and for this reason, these compounds are safer in comparison.[227] Other relatives of ethanol with similar effects include chloral hydrate, paraldehyde, and many volatile and inhalational anesthetics (e.g., chloroform, diethyl ether, and isoflurane).
The Lucas test differentiates between primary, secondary, and tertiary alcohols.
Ethchlorvynol is not compatible with intravenous injection like ethanol—serious injury (including the loss of limbs due to vascular injury) or death can occur when it is used in this manner.[228]
Society and culture edit
Usage edit
Consumption recommendations edit

The recommended maximum intake (or safe limits) of alcohol varies from no intake, to daily, weekly, or daily/weekly guidelines provided by health agencies of governments. The World Health Organization published a statement in The Lancet Public Health in April 2023 that "there is no safe amount that does not affect health".[20]
According to a 2024 systematic review and meta-analysis, even at 20 g/day (1 large beer), the risk of developing an alcohol use disorder (AUD) is nearly 3 times higher than non-drinkers, and the risk of dying from an AUD is about 2 times higher than non-drinkers.[229]
Drinking culture edit

Ethanol is typically consumed as a recreational substance by mouth in the form of alcoholic beverages such as beer, wine, and spirits. It is commonly used in social settings due to its capacity to enhance sociability.
Drinking alcohol is generally socially acceptable and is legal in most countries, unlike with many other recreational substances. Many students attending colleges, universities, and other higher education institutions consume alcoholic beverages. However, there are often restrictions on alcohol sale and use, for instance a minimum age for drinking and laws against public drinking and drinking and driving.[230] Alcohol has considerable societal and cultural significance and has important social roles in much of the world. Drinking establishments, such as bars and nightclubs, revolve primarily around the sale and consumption of alcoholic beverages, and parties, festivals, and social gatherings commonly involve alcohol consumption. Alcohol is related to various societal problems, including drunk driving, accidental injuries, sexual assaults, domestic abuse, and violent crime.[92] Alcohol remains illegal for sale and consumption in a number of countries, mainly in the Middle East.
Research on the societal benefits of alcohol is rare, but a 2017 study suggested there are benefits.[231] Alcohol is often used as a social lubricant; it increases occurrences of Duchenne smiling, talking, and social bonding, even when participants are unaware of their alcohol consumption or lack thereof.[232] In a study of the UK, regular drinking was correlated with happiness, feeling that life was worthwhile, and life satisfaction. According to a causal path analysis the cause was vice versa; alcohol consumption was not the cause, but rather that the life satisfaction resulted in greater happiness and an inclination to visit pubs and develop a regular drinking venue. City centre bars were distinguished by their focus on maximizing alcohol sales. Community pubs had less variation in visible group sizes and longer, more focused conversations than those in city centre bars. Drinking regularly at a community pub led to higher trust in others and better networking with the local community, compared to non-drinkers and city centre bar drinkers.[231]
Religion edit

The relationship between alcohol and religion exhibits variations across cultures, geographical areas, and religious denominations. Some religions emphasize moderation and responsible use as a means of honoring the divine gift of life, while others impose outright bans on alcohol as a means of honoring the divine gift of life. Moreover, within the same religious tradition, there are many adherents that may interpret and practice their faith's teachings on alcohol in diverse ways. Hence, a wide range of factors, such as religious affiliation, levels of religiosity, cultural traditions, family influences, and peer networks, collectively influence the dynamics of this relationship.
The levels of alcohol use in spiritual context can be broken down into:
- Prohibition: Some religions, including Islam[233] prohibit alcohol consumption.
- Symbolic use: In some Christian denominations, the sacramental wine is alcoholic, however, only a sip is taken, and it does not raise the blood alcohol content, and other denominations are using nonalcoholic wine. See also Libation.
- Discourage consumption: Hinduism does not have a central authority which is followed by all Hindus, though religious texts generally discourage the use or consumption of alcohol.
- Entheogenic use: See the spiritual section.
- Recreational use: Recreational drug use of alcohol in moderation to celebrate joy, is allowed in some religions.
- Christian views on alcohol are varied. For example, in the mid-19th century, some Protestant Christians moved from a position of allowing moderate use of alcohol (sometimes called moderationism) to either deciding that not imbibing was wisest in the present circumstances (abstentionism) or prohibiting all ordinary consumption of alcohol because it was believed to be a sin (prohibitionism).[234]
- During the Jewish holiday of Purim, Jews are obligated to drink (especially Kosher wine) until their judgmental abilities become impaired according to the Book of Esther.[235][236][237] However, Purim has more of a national than a religious character.
Law edit
Legal status edit

Alcohol consumption is fully legal and available in most countries of the world.[238] Home made alcoholic beverages with low alcohol content like wine, and beer is also legal in most countries, but distilling moonshine outside of a registered distillery remains illegal in most of them.
Some majority-Muslim countries, such as Saudi Arabia, Kuwait, Pakistan, Iran and Libya prohibit the production, sale, and consumption of alcoholic beverages because they are forbidden by Islam.[239][240][241] Laws banning alcohol consumption are found in some Indian states as well as some Native American reservations in the U.S.[238]
In addition, there are regulations on alcohol sales and use in many countries throughout the world.[238] For instance, the majority of countries have a minimum legal drinking age to purchase or consume alcoholic beverages, although there are often exceptions such as underage consumption of small amounts of alcohol with parental supervision. Also, some countries have bans on public intoxication.[238] Drinking while driving or intoxicated driving is frequently outlawed and it may be illegal to have an open container of alcohol or liquor bottle in an automobile, bus or aircraft.[238]
In Iran, consumption of alcohol (one glass) is punished by 80 lashes, but repeated offences may lead to death penalty, although rarely exercised. In 2012, two men were sentenced to death after a third offense in Khorasan.[242][243]
Alcohol packaging warning messages edit

Alcohol packaging warning messages (alcohol warning labels, AWLs[244]) are warning messages that appear on the packaging of alcoholic drinks concerning their health effects.
A World Health Organization report, published in 2017, stated:[245]
Alcohol product labelling could be considered as a component of a comprehensive public health strategy to reduce alcohol-related harm. Adding health labels to alcohol containers is an important first step in raising awareness and has a longer-term utility in helping to establish a social understanding of the harmful use of alcohol.
Criticism of the alcohol industry edit

A 2019 survey conducted by the American Institute for Cancer Research (AICR) showed that only 45% of Americans were aware of the associated risk of cancer due to alcohol consumption, up from 39% in 2017.[246] The AICR believes that alcohol-related advertisements about the healthy cardiovascular benefits of modest alcohol overshadow messages about the increased cancer risks.[246]
Drinking alcoholic beverages increase the risk for breast cancer. Several studies indicate that the use of marketing by the alcohol industry to associate their products with breast cancer awareness campaigns, known as pinkwashing, is misleading and potentially harmful.[247][248][249][250]
The alcohol industries have marketed products directly to the LGBT+ community. In 2010, of the sampled parades that listed sponsors, 61% of the prides were sponsored by the alcohol industry.[251]
Standard drink edit
A standard drink is a measure of alcohol consumption representing a fixed amount of pure ethanol, used in relation to recommendations about alcohol consumption and its relative risks to health. The size of a standard drink varies from 8g to 20g across countries, but 10g alcohol (12.7 millilitres) is used in the World Health Organization (WHO) Alcohol Use Disorders Identification Test (AUDIT)'s questionnaire form example,[252] and has been adopted by more countries than any other amount.[253]
Sober curious edit

Source: SAMHSA[254]
Sober curious is a cultural movement and lifestyle of consuming no or limited alcohol that started in the late 2010s.[citation needed] It differs from traditional abstinence in that it is not founded on asceticism, religious condemnation of alcohol or previous alcohol abuse, but motivated by a curiosity of a sober lifestyle. Markets have reacted by offering a wider selection of non-alcoholic beverages.[255]
Sober curiosity is often defined as having the option to question or change one's drinking habits, for mental or physical health reasons.[256] It may be practised in many ways, ranging from complete abstinence to more thought about when and how much is consumed.[257]
Since the onset of the COVID-19 pandemic, more people in Europe have reduced their alcohol consumption.[258]
History edit
Early modern period edit

The Gin Craze was a period in the first half of the 18th century when the consumption of gin increased rapidly in Great Britain, especially in London. By 1743, England was drinking 2.2 gallons (10 litres) of gin per person per year. The Sale of Spirits Act 1750 (commonly known as the Gin Act 1751) was an Act of the Parliament of Great Britain (24 Geo. 2. c. 40) which was enacted in order to reduce the consumption of gin and other distilled spirits, a popular pastime[259]
Modern period edit
The Andrew Johnson alcoholism debate is the dispute, originally conducted amongst the general public, and now typically a question for historians, about whether or not Andrew Johnson, the 17th president of the United States (1865–1869), drank to excess.
The Bratt System was a system that was used in Sweden (1919–1955) and similarly in Finland (1944–1970) to control alcohol consumption, by rationing of liquor. Every citizen allowed to consume alcohol was given a booklet called a motbok (viinakortti in Finland), in which a stamp was added each time a purchase was made at Systembolaget (in Sweden) and Alko (in Finland).[260] A similar system also existed in Estonia between July 1, 1920 to December 31, 1925.[261] The stamps were based on the amount of alcohol bought. When a certain amount of alcohol had been bought, the owner of the booklet had to wait until next month to buy more.
The Medicinal Liquor Prescriptions Act of 1933 was a law passed by Congress in response to the abuse of medicinal liquor prescriptions during Prohibition.
The rum ration (also called the tot) was a daily amount of rum given to sailors on Royal Navy ships. It was abolished in 1970 after concerns that the intake of strong alcohol would lead to unsteady hands when working machinery.
See also edit
- Binge drinking
- Alcohol myopia
- Rum-running
- Responsible drug use
- GABAergics
- GABRD (δ subunit-containing receptors)
- List of countries by alcohol consumption per capita
- Pigovian taxes, which are to pay for the damage to society caused by these goods.
- Sin taxes are used to increase the price in an effort to lower their use, or failing that, to increase and find new sources of revenue.
References edit
- ^ WHO Expert Committee on Problems Related to Alcohol Consumption : second report. Geneva, Switzerland: World Health Organization. 2007. p. 23. ISBN 978-92-4-120944-1. Retrieved 3 March 2015.
...alcohol dependence (is) a substantial risk of regular heavy drinking...
- ^ Vengeliene V, Bilbao A, Molander A, Spanagel R (May 2008). "Neuropharmacology of alcohol addiction". British Journal of Pharmacology. 154 (2): 299–315. doi:10.1038/bjp.2008.30. PMC 2442440. PMID 18311194.
(Compulsive alcohol use) occurs only in a limited proportion of about 10–15% of alcohol users....
- ^ Gilman JM, Ramchandani VA, Crouss T, Hommer DW (January 2012). "Subjective and neural responses to intravenous alcohol in young adults with light and heavy drinking patterns". Neuropsychopharmacology. 37 (2): 467–77. doi:10.1038/npp.2011.206. PMC 3242308. PMID 21956438.
- ^ a b c d e f g h i j k l m n o p q r s t u Principles of Addiction: Comprehensive Addictive Behaviors and Disorders. Academic Press. 17 May 2013. pp. 162–. ISBN 978-0-12-398361-9.
- ^ a b c d e f g h i Holford NH (November 1987). "Clinical pharmacokinetics of ethanol". Clinical Pharmacokinetics. 13 (5): 273–92. doi:10.2165/00003088-198713050-00001. PMID 3319346. S2CID 19723995.
- ^ a b c d e f g h i j k l m n o p q r s t u v w Pohorecky LA, Brick J (1988). "Pharmacology of ethanol". Pharmacology & Therapeutics. 36 (2–3): 335–427. doi:10.1016/0163-7258(88)90109-x. PMID 3279433.
- ^ a b Becker CE (September 1970). "The clinical pharmacology of alcohol". California Medicine. 113 (3): 37–45. PMC 1501558. PMID 5457514.
- ^ a b c d e f g h i Levine B (2003). Principles of Forensic Toxicology. Amer. Assoc. for Clinical Chemistry. pp. 161–. ISBN 978-1-890883-87-4.
- ^ Iber FL (26 November 1990). Alcohol and Drug Abuse as Encountered in Office Practice. CRC Press. pp. 74–. ISBN 978-0-8493-0166-7.
- ^ a b c Haynes WM, ed. (2011). CRC Handbook of Chemistry and Physics (92nd ed.). Boca Raton, FL: CRC Press. p. 3.246. ISBN 1-4398-5511-0.
- ^ a b c Collins SE, Kirouac M (2013). "Alcohol Consumption". Encyclopedia of Behavioral Medicine. pp. 61–65. doi:10.1007/978-1-4419-1005-9_626. ISBN 978-1-4419-1004-2.
- ^ Różański M, Pielech-Przybylska K, Balcerek M (September 2020). "Influence of Alcohol Content and Storage Conditions on the Physicochemical Stability of Spirit Drinks". Foods. 9 (9): 1264. doi:10.3390/foods9091264. PMC 7555269. PMID 32916918.
- ^ "17.7: Oxidation of Alcohols". Chemistry LibreTexts. 26 August 2015.
- ^ Burcham PC (19 November 2013). An Introduction to Toxicology. Springer Science & Business Media. pp. 42–. ISBN 978-1-4471-5553-9.
- ^ a b "Agents Classified by the IARC Monographs, Volumes 1–111" (PDF). Archived from the original (PDF) on 25 October 2011 – via monographs.iarc.fr.
- ^ Heaton MB, Mitchell JJ, Paiva M (April 2000). "Amelioration of ethanol-induced neurotoxicity in the neonatal rat central nervous system by antioxidant therapy". Alcoholism: Clinical and Experimental Research. 24 (4): 512–18. doi:10.1111/j.1530-0277.2000.tb02019.x. PMID 10798588.
- ^ Brust JC (April 2010). "Ethanol and cognition: indirect effects, neurotoxicity and neuroprotection: a review". International Journal of Environmental Research and Public Health. 7 (4): 1540–57. doi:10.3390/ijerph7041540. PMC 2872345. PMID 20617045.
- ^ a b Popova S, Dozet D, Shield K, Rehm J, Burd L (September 2021). "Alcohol's Impact on the Fetus". Nutrients. 13 (10): 3452. doi:10.3390/nu13103452. PMC 8541151. PMID 34684453.
- ^ a b Chung DD, Pinson MR, Bhenderu LS, Lai MS, Patel RA, Miranda RC (August 2021). "Toxic and Teratogenic Effects of Prenatal Alcohol Exposure on Fetal Development, Adolescence, and Adulthood". International Journal of Molecular Sciences. 22 (16): 8785. doi:10.3390/ijms22168785. PMC 8395909. PMID 34445488.
- ^ a b "No level of alcohol consumption is safe for our health". World Health Organization. 4 January 2023.
- ^ a b Nutt DJ, King LA, Phillips LD (November 2010). "Drug harms in the UK: a multicriteria decision analysis". Lancet. 376 (9752): 1558–65. CiteSeerX 10.1.1.690.1283. doi:10.1016/S0140-6736(10)61462-6. PMID 21036393. S2CID 5667719.
- ^ a b Park SH, Kim DJ (October 2020). "Global and regional impacts of alcohol use on public health: Emphasis on alcohol policies". Clinical and Molecular Hepatology. 26 (4): 652–661. doi:10.3350/cmh.2020.0160. PMC 7641561. PMID 33053937.
- ^ a b c Mathurin P, Deltenre P (May 2009). "Effect of binge drinking on the liver: an alarming public health issue?". Gut. 58 (5): 613–17. doi:10.1136/gut.2007.145573. PMID 19174416. S2CID 43370272.
- ^ a b de Menezes RF, Bergmann A, Thuler LC (2013). "Alcohol consumption and risk of cancer: a systematic literature review". Asian Pacific Journal of Cancer Prevention. 14 (9): 4965–72. doi:10.7314/apjcp.2013.14.9.4965. PMID 24175760.
- ^ Bagnardi V, Rota M, Botteri E, Tramacere I, Islami F, Fedirko V, et al. (February 2013). "Light alcohol drinking and cancer: a meta-analysis". Annals of Oncology. 24 (2): 301–8. doi:10.1093/annonc/mds337. PMID 22910838.
- ^ Yasinski E (12 January 2021). "Even If You Don't Drink Daily, Alcohol Can Mess With Your Brain". Discover.
- ^ a b c d e f g h i j k l m Lobo IA, Harris RA (July 2008). "GABA(A) receptors and alcohol". Pharmacology Biochemistry and Behavior. 90 (1): 90–94. doi:10.1016/j.pbb.2008.03.006. PMC 2574824. PMID 18423561.
- ^ a b c d e Narahashi T, Kuriyama K, Illes P, Wirkner K, Fischer W, Mühlberg K, et al. (May 2001). "Neuroreceptors and ion channels as targets of alcohol". Alcoholism: Clinical and Experimental Research. 25 (5 Suppl ISBRA): 182S–188S. doi:10.1097/00000374-200105051-00030. PMID 11391069.
- ^ a b c d Olsen RW, Li GD, Wallner M, Trudell JR, Bertaccini EJ, Lindahl E, et al. (March 2014). "Structural models of ligand-gated ion channels: sites of action for anesthetics and ethanol". Alcoholism: Clinical and Experimental Research. 38 (3): 595–603. doi:10.1111/acer.12283. PMC 3959612. PMID 24164436.
- ^ Charlet K, Beck A, Heinz A (2013). "The dopamine system in mediating alcohol effects in humans". Current Topics in Behavioral Neurosciences. 13: 461–88. doi:10.1007/7854_2011_130. ISBN 978-3-642-28719-0. PMID 21533679.
- ^ Méndez M, Morales-Mulia M (June 2008). "Role of mu and delta opioid receptors in alcohol drinking behaviour". Current Drug Abuse Reviews. 1 (2): 239–52. doi:10.2174/1874473710801020239. PMID 19630722.
- ^ Yang C, Latkin C, Luan R, Nelson K (February 2013). "Factors associated with drinking alcohol before visiting female sex workers among men in Sichuan Province, China". AIDS and Behavior. 17 (2): 568–573. doi:10.1007/s10461-012-0260-8. PMC 4017933. PMID 22806054.
- ^ Beksinska A, Karlsen O, Gafos M, Beattie TS (2023). "Alcohol use and associated risk factors among female sex workers in low- and middle-income countries: A systematic review and meta-analysis". PLOS Global Public Health. 3 (6): e0001216. doi:10.1371/journal.pgph.0001216. PMC 10263362. PMID 37310993.
- ^ "Dutch". Oxford English Dictionary (2nd ed.). Oxford University Press. 1989.
- ^ Byrne E (26 July 2013). "What is the origin of the phrase 'Dutch Courage'?". History Extra. Retrieved 26 December 2022.
- ^ Martin G. "Dutch courage". Phrases. UK. Retrieved 26 December 2022.
- ^ Jones E, Fear NT (April 2011). "Alcohol use and misuse within the military: a review". International review of psychiatry (Abingdon, England). 23 (2): 166–72. doi:10.3109/09540261.2010.550868. PMID 21521086.
- ^ Dworkin ER, Bergman HE, Walton TO, Walker DD, Kaysen DL (2018). "Co-Occurring Post-Traumatic Stress Disorder and Alcohol Use Disorder in U.S. Military and Veteran Populations". Alcohol research : current reviews. 39 (2): 161–169. PMC 6561402. PMID 31198655.
- ^ Osborne VA, Sher KJ, Winograd RP (2011). "Disordered eating patterns and alcohol misuse in college students: Evidence for "drunkorexia"?". Comprehensive Psychiatry. 52 (6): e12. doi:10.1016/j.comppsych.2011.04.038.
- ^ "'Drunkorexia:' A Recipe for Disaster". ScienceDaily. 17 October 2011.
- ^ "Composition of Foods Raw, Processed, Prepared USDA National Nutrient Database for Standard Reference, Release 26 Documentation and User Guide" (PDF). USDA. August 2013. p. 14. Archived (PDF) from the original on 25 September 2014. Retrieved 3 February 2014.
- ^ "What We Eat in America, NHANES 2013-2014" (PDF). Archived (PDF) from the original on 24 February 2017. Retrieved 29 September 2021.
- ^ Metz R, Berger S, Mako M (August 1969). "Potentiation of the plasma insulin response to glucose by prior administration of alcohol. An apparent islet-priming effect" (PDF). Diabetes. 18 (8): 517–522. doi:10.2337/diab.18.8.517. PMID 4897290. S2CID 32072796. Archived (PDF) from the original on 22 February 2014. Retrieved 11 February 2014.
- ^ Shelmet JJ, Reichard GA, Skutches CL, Hoeldtke RD, Owen OE, Boden G (April 1988). "Ethanol causes acute inhibition of carbohydrate, fat, and protein oxidation and insulin resistance". The Journal of Clinical Investigation. 81 (4): 1137–1145. doi:10.1172/JCI113428. PMC 329642. PMID 3280601.
- ^ Mégarbane B (24 August 2010). "Treatment of patients with ethylene glycol or methanol poisoning: focus on fomepizole". Open Access Emergency Medicine. 2: 67–75. doi:10.2147/OAEM.S5346. PMC 4806829. PMID 27147840.
- ^ British National Formulary: BNF 69 (69th ed.). British Medical Association. 2015. pp. 42, 838. ISBN 978-0-85711-156-2.
- ^ Barceloux DG, Bond GR, Krenzelok EP, Cooper H, Vale JA (2002). "American Academy of Clinical Toxicology practice guidelines on the treatment of methanol poisoning". Journal of Toxicology. Clinical Toxicology. 40 (4): 415–46. doi:10.1081/CLT-120006745. PMID 12216995. S2CID 26495651.
- ^ "Our 'drinking culture' explored". www.linkedin.com. Retrieved 25 January 2024.
- ^ Gable RS (June 2004). "Comparison of acute lethal toxicity of commonly abused psychoactive substances" (PDF). Addiction. 99 (6): 686–96. doi:10.1111/j.1360-0443.2004.00744.x. PMID 15139867.
- ^ Riley JL 3rd, King C (September 2009). "Self-report of alcohol use for pain in a multi-ethnic community sample". The Journal of Pain. 10 (9): 944–52. doi:10.1016/j.jpain.2009.03.005. PMC 2734914. PMID 19712901.
- ^ Sarah W. Book and Carrie L. Randall Social anxiety disorder and alcohol use. Alcohol Research and Health, 2002.
- ^ Wetterling T, Junghanns K (December 2000). "Psychopathology of alcoholics during withdrawal and early abstinence". Eur Psychiatry. 15 (8): 483–88. doi:10.1016/S0924-9338(00)00519-8. PMID 11175926. S2CID 24094651.
- ^ Cowley DS (1 January 1992). "Alcohol abuse, substance abuse, and panic disorder". Am J Med. 92 (1A): 41S–8S. doi:10.1016/0002-9343(92)90136-Y. PMID 1346485.
- ^ Cosci F, Schruers KR, Abrams K, Griez EJ (June 2007). "Alcohol use disorders and panic disorder: a review of the evidence of a direct relationship". J Clin Psychiatry. 68 (6): 874–80. doi:10.4088/JCP.v68n0608. PMID 17592911.
- ^ Müller CP, Schumann G, Rehm J, Kornhuber J, Lenz B (July 2023). "Self-management with alcohol over lifespan: psychological mechanisms, neurobiological underpinnings, and risk assessment". Molecular Psychiatry. 28 (7): 2683–2696. doi:10.1038/s41380-023-02074-3. PMC 10615763. PMID 37117460.
- ^ "Alcohol & Sleep: Nix the Nightcap?". Webmd. Retrieved 1 November 2015.
- ^ Penning R, van Nuland M, Fliervoet LA, Olivier B, Verster JC (June 2010). "The pathology of alcohol hangover". Current Drug Abuse Reviews. 3 (2): 68–75. doi:10.2174/1874473711003020068. PMID 20712596.
- ^ Wiese JG, Shlipak MG, Browner WS (June 2000). "The alcohol hangover". Annals of Internal Medicine. 132 (11): 897–902. doi:10.7326/0003-4819-132-11-200006060-00008. PMID 10836917.
- ^ Breene S (6 October 2016). "The best and worst foods to cure a hangover". The Atlanta Journal-Constitution. Retrieved 30 July 2017.
- ^ Acocella J (26 May 2008). "A Few Too Many: Is there any hope for the hung over?". The New Yorker.
- ^ Harding A (21 December 2010). "10 Hangover Remedies: What Works?". Health.com. Retrieved 30 July 2017.
- ^ Howard J (17 March 2017). "What to eat to beat a hangover". CNN. Retrieved 30 July 2017.
- ^ "Myth busters". who.int. World Health Organization.
- ^ Baumgarten A. "10 common myths busted about coronavirus in North Dakota". The Dickinson Press. Retrieved 14 April 2020.
- ^ Szabo G, Saha B (2015). "Alcohol's Effect on Host Defense". Alcohol Research. 37 (2): 159–170. PMC 4590613. PMID 26695755.
- ^ Soileau M (August 2012). "Spreading the Sofra: Sharing and Partaking in the Bektashi Ritual Meal". History of Religions. 52 (1): 1–30. doi:10.1086/665961. JSTOR 10.1086/665961. Retrieved 5 June 2021.
- ^ Bocking B (1997). A popular dictionary of Shintō (Rev. ed.). Richmond, Surrey [U.K.]: Curzon Press. ISBN 0-7007-1051-5. OCLC 264474222.
- ^ "More than 3 million US women at risk for alcohol-exposed pregnancy". Centers for Disease Control and Prevention. 2 February 2016. Retrieved 3 March 2016.
'drinking any alcohol at any stage of pregnancy can cause a range of disabilities for their child,' said Coleen Boyle, Ph.D., director of CDC's National Center on Birth Defects and Developmental Disabilities.
- ^ "Civil Commitment: About This Policy". Alcohol Policy Information System. NIAAA. Retrieved 15 March 2024.
- ^ a b c d e Friedman HS (26 August 2011). The Oxford Handbook of Health Psychology. Oxford University Press, USA. pp. 699–. ISBN 978-0-19-534281-9.
- ^ "No level of alcohol consumption is safe for our health". www.who.int. Retrieved 13 October 2023.
- ^ Reimold D (29 May 2012). "College Word of the Year Contest contenders: Drunkorexia, shmacked and FOMO". The Washington Post. Retrieved 16 November 2012.
- ^ a b Alcohol-Related Psychosis at eMedicine
- ^ Tien AY, Anthony JC (August 1990). "Epidemiological analysis of alcohol and drug use as risk factors for psychotic experiences". The Journal of Nervous and Mental Disease. 178 (8): 473–480. doi:10.1097/00005053-199017880-00001. PMID 2380692.
- ^ Cargiulo T (March 2007). "Understanding the health impact of alcohol dependence". American Journal of Health-System Pharmacy. 64 (5 Suppl 3): S5-11. doi:10.2146/ajhp060647. PMID 17322182.
- ^ Schuckit MA (November 1983). "Alcoholism and other psychiatric disorders". Hospital & Community Psychiatry. 34 (11): 1022–1027. doi:10.1176/ps.34.11.1022. PMID 6642446.
- ^ Monnot, M., Nixon, S., Lovallo, W., & Ross, E. (2001). Altered emotional perception in alcoholics: Deficits in affective prosody comprehension. [Article]. Alcoholism: Clinical and Experimental Research, 25(3), 362-369.
- ^ a b Hendler RA, Ramchandani VA, Gilman J, Hommer DW (2013). "Stimulant and sedative effects of alcohol". Current Topics in Behavioral Neurosciences. 13: 489–509. doi:10.1007/7854_2011_135. ISBN 978-3-642-28719-0. PMID 21560041.
- ^ Peters GL, Rosselli JL, Kerr JL. "Overview of Peptic Ulcer Disease: Etiology and Pathophysiology". Medscape.com. Retrieved 27 April 2013.
- ^ a b Dumain T. Pathak N (ed.). "Peptic Ulcer Disease (Stomach Ulcers) Cause, Symptoms, Treatments". Webmd.com. Retrieved 27 April 2013.
- ^ Patel S, Behara R, Swanson GR, Forsyth CB, Voigt RM, Keshavarzian A (October 2015). "Alcohol and the Intestine". Biomolecules. 5 (4): 2573–88. doi:10.3390/biom5042573. PMC 4693248. PMID 26501334.
- ^ Jain A, Yelamanchili VS, Brown KN, Goel A (2024). "Holiday Heart Syndrome". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 30725870. Retrieved 15 February 2024.
- ^ "Holiday heart syndrome – definition". Biology-Online.org.
- ^ Rosenthal L, Stokken GT, Smith RH, Daubert JP, Weiss HS, Budzikowski AS (17 October 2021). Talavera F, Compton SJ, Dizon JM (eds.). "Holiday Heart Syndrome: Background, Pathophysiology, Epidemiology". Medscape.
- ^ Ettinger PO, Wu CF, De La Cruz C, Weisse AB, Ahmed SS, Regan TJ (May 1978). "Arrhythmias and the "Holiday Heart": alcohol-associated cardiac rhythm disorders". American Heart Journal. 95 (5): 555–562. doi:10.1016/0002-8703(78)90296-x. PMID 636996.
- ^ Tonelo D, Providência R, Gonçalves L (August 2013). "Holiday heart syndrome revisited after 34 years". Arquivos Brasileiros de Cardiologia. 101 (2): 183–189. doi:10.5935/abc.20130153. PMC 3998158. PMID 24030078.
- ^ Brown KN, Yelamanchili VS, Goel A (2022). "Holiday Heart Syndrome". StatPearls. Treasure Island (FL): StatPearls Publishing. PMID 30725870. Retrieved 26 August 2022.
- ^ K. E. Money, W. S. Myles (8 February 1974). "Heavy water nystagmus and effects of alcohol". Nature. 247 (5440): 404–405. Bibcode:1974Natur.247..404M. doi:10.1038/247404a0. PMID 4544739. S2CID 4166559.
- ^ Brooks PJ, Enoch MA, Goldman D, Li TK, Yokoyama A (March 2009). "The alcohol flushing response: an unrecognized risk factor for esophageal cancer from alcohol consumption". PLOS Medicine. 6 (3): e50. doi:10.1371/journal.pmed.1000050. PMC 2659709. PMID 19320537.
- ^ McMurran M (3 October 2012). Alcohol-Related Violence: Prevention and Treatment. John Wiley & Sons. p. 37. ISBN 978-1-118-41106-3.
- ^ Adams KE, Rans TS (December 2013). "Adverse reactions to alcohol and alcoholic beverages". Annals of Allergy, Asthma & Immunology. 111 (6): 439–45. doi:10.1016/j.anai.2013.09.016. PMID 24267355.
- ^ a b c d e f g h i j k l m n o p Butcher JN, Hooley JM, Mineka SM (25 June 2013). Abnormal Psychology. Pearson Education. p. 370. ISBN 978-0-205-97175-6.
- ^ Bakalar N (27 August 2018). "How Much Alcohol Is Safe to Drink? None, Say These Researchers". The New York Times. Retrieved 17 September 2018.
- ^ Tomlinson A (26 June 2018). "Tips and Tricks on How to Cut Down on the Booze". The West Australian. Seven West Media (WA). Retrieved 22 March 2019.
- ^ "Alcohol". British Liver Trust. Archived from the original on 11 July 2019. Retrieved 22 March 2019.
- ^ "What to Know About Dry Drunk Syndrome".
- ^ David W. Brook, Henry I. Spitz (23 September 2002). The Group Therapy of Substance Abuse. CRC Press. p. 73. ISBN 978-0-7890-1782-6.
- ^ Benton SA (2009). Understanding the High-Functioning Alcoholic – Professional Views and Personal Insights. Greenwood Publishing Group. ISBN 978-0-313-35280-5.
- ^ Brody J (4 May 2009). "High Functioning, but Still Alcoholics". The New York Times. Retrieved 18 February 2012.
- ^ "What is a High Functioning Alcoholic? | Definition & Signs". Alcohol.org. Retrieved 29 January 2021.
- ^ Szlemko WJ, Wood JW, Thurman PJ (October 2006). "Native Americans and alcohol: past, present, and future". The Journal of General Psychology. 133 (4). Heldref Publications: 435–451. doi:10.3200/GENP.133.4.435-451. PMID 17128961. S2CID 43082343.
- ^ Ashworth M, Gerada C (August 1997). "ABC of mental health. Addiction and dependence – II: Alcohol". BMJ. 315 (7104): 358–360. doi:10.1136/bmj.315.7104.358. PMC 2127236. PMID 9270461.
- ^ Fisher GL, Roget NA, eds. (2009). "Withdrawal: Alcohol". Encyclopedia of substance abuse prevention, treatment, & recovery. Los Angeles: SAGE. p. 1005. ISBN 978-1-4522-6601-5. Archived from the original on 22 December 2015.
- ^ McClure EA, Gipson CD, Malcolm RJ, Kalivas PW, Gray KM (2014). "Potential role of N-acetylcysteine in the management of substance use disorders". CNS Drugs. 28 (2): 95–106. doi:10.1007/s40263-014-0142-x. PMC 4009342. PMID 24442756.
- ^ Allison MG, McCurdy MT (May 2014). "Alcoholic metabolic emergencies". Emergency Medicine Clinics of North America. 32 (2): 293–301. doi:10.1016/j.emc.2013.12.002. PMID 24766933.
- ^ Howard RD, Bokhari S (January 2019). Alcoholic Ketoacidosis (AKA). PMID 28613672.
- ^ a b McGuire LC, Cruickshank AM, Munro PT (June 2006). "Alcoholic ketoacidosis". Emergency Medicine Journal. 23 (6): 417–420. doi:10.1136/emj.2004.017590. PMC 2564331. PMID 16714496.
- ^ Ridley NJ, Draper B, Withall A (25 January 2013). "Alcohol-related dementia: an update of the evidence". Alzheimer's Research & Therapy. 5 (1): 3. doi:10.1186/alzrt157. PMC 3580328. PMID 23347747.
- ^ Piano MR (May 2002). "Alcoholic cardiomyopathy: incidence, clinical characteristics, and pathophysiology". Chest. 121 (5): 1638–50. doi:10.1378/chest.121.5.1638. PMC 1923411. PMID 12006456.
- ^ Georgiadou SP, Manoulakas E, Makaritsis KP, Dalekos GN (May 2018). "A chronic alcoholic man with high fever, neck rigidity and loss of consciousness: remember the Austrian syndrome a commonly unrecognised invasive pneumococcus triad". BMJ Case Reports. 2018: bcr–2018–225010. doi:10.1136/bcr-2018-225010. PMC 5976089. PMID 29848535.
- ^ "10th Special Report to the U.S. Congress on Alcohol and Health: Highlights from Current Research" (PDF). National Institute of Health. National Institute on Alcohol Abuse and Alcoholism. June 2000. p. 134. Archived from the original (PDF) on 21 February 2016. Retrieved 21 October 2014.
The brain is a major target for the actions of alcohol, and heavy alcohol consumption has long been associated with brain damage. Studies clearly indicate that alcohol is neurotoxic, with direct effects on nerve cells. Chronic alcohol abusers are at additional risk for brain injury from related causes, such as poor nutrition, liver disease, and head trauma.
- ^ a b Arts NJ, Walvoort SJ, Kessels RP (27 November 2017). "Korsakoff's syndrome: a critical review". Neuropsychiatric Disease and Treatment. 13: 2875–2890. doi:10.2147/NDT.S130078. PMC 5708199. PMID 29225466.
- ^ "Report Details Alcohol's Global Cancer Burden - NCI". www.cancer.gov. 12 August 2021. Retrieved 13 October 2023.
- ^ Bruha R, Dvorak K, Petrtyl J (March 2012). "Alcoholic liver disease". World Journal of Hepatology. 4 (3): 81–90. doi:10.4254/wjh.v4.i3.81. PMC 3321494. PMID 22489260.
- ^ "Neonatal abstinence Syndrome". MedlinePlus. US Library of Medicine. 2017. Retrieved 27 July 2017.
 This article incorporates text from this source, which is in the public domain.
This article incorporates text from this source, which is in the public domain.
- ^ "Triglycerides". American Heart Association. Archived from the original on 27 August 2007. Retrieved 4 September 2007.
- ^ Nutt D, King LA, Saulsbury W, Blakemore C (March 2007). "Development of a rational scale to assess the harm of drugs of potential misuse". Lancet. 369 (9566): 1047–53. doi:10.1016/s0140-6736(07)60464-4. PMID 17382831. S2CID 5903121.
- ^ Cheng B, Lim CC, Rutherford BN, Huang S, Ashley DP, Johnson B, et al. (January 2024). "A systematic review and meta-analysis of the relationship between youth drinking, self-posting of alcohol use and other social media engagement (2012-21)". Addiction. 119 (1): 28–46. doi:10.1111/add.16304. PMID 37751678.
- ^ a b c d e f g h Sunga HE (2016). "Alcohol and Crime". The Blackwell Encyclopedia of Sociology. American Cancer Society. pp. 1–2. doi:10.1002/9781405165518.wbeosa039.pub2. ISBN 978-1-4051-6551-8.
- ^ Borsari B, Murphy JG, Barnett NP (October 2007). "Predictors of alcohol use during the first year of college: implications for prevention". Addictive Behaviors. 32 (10): 2062–2086. doi:10.1016/j.addbeh.2007.01.017. PMC 2614076. PMID 17321059.
- ^ Amiri S (April 2022). "Smoking and alcohol use in unemployed populations: a systematic review and meta-analysis". Journal of Addictive Diseases. 40 (2): 254–277. doi:10.1080/10550887.2021.1981124. PMID 34747337.
- ^ Trevor B, Katy H (1 April 2005). Understanding Drugs, Alcohol And Crime. McGraw-Hill Education (UK). p. 6. ISBN 978-0-335-21257-6.
- ^ "Drunk Driving Statistics in the US and Across the World". Law Office of Douglas Herring. 13 November 2017. Archived from the original on 22 September 2019. Retrieved 22 September 2019.
- ^ "Drunk Driving Increasing Concern Worldwide". Voice of America. Retrieved 22 September 2019.
- ^ Sweedler BM, Stewart K (2009). "Worldwide trends in alcohol and drug impaired driving". In Verster JC, Pandi-Perumal SR, Ramaekers JG, de Gier JJ (eds.). Drugs, Driving and Traffic Safety. Birkhäuser Basel. pp. 23–41. doi:10.1007/978-3-7643-9923-8_2. ISBN 978-3-7643-9923-8.
- ^ a b c d Clinard M, Meier R (14 February 2007). Sociology of Deviant Behavior. Cengage Learning. p. 273. ISBN 978-0-495-09335-0.
- ^ a b McMurran M (3 October 2012). Alcohol-Related Violence: Prevention and Treatment. John Wiley & Sons. pp. 337–338. ISBN 978-1-118-41106-3.
- ^ a b c McMurran M (3 October 2012). Alcohol-Related Violence: Prevention and Treatment. John Wiley & Sons. p. 37. ISBN 978-1-118-41106-3.
- ^ "WHO | Governments confront drunken violence". WHO. Archived from the original on 4 May 2014. Retrieved 22 September 2019.
- ^ a b "Global status report on alcohol and health" (PDF). World Health Organization. 2011.
- ^ Smith R (16 March 2010). "'Passive drinking' is blighting the nation, Sir Liam Donaldson warns". The Daily Telegraph. Archived from the original on 20 March 2009. Retrieved 30 May 2010.
- ^ Hingson R, Winter M (2003). "Epidemiology and consequences of drinking and driving". Alcohol Research & Health. 27 (1): 63–78. PMC 6676697. PMID 15301401.
- ^ Naranjo CA, Bremner KE (January 1993). "Behavioural correlates of alcohol intoxication". Addiction. 88 (1): 25–35. doi:10.1111/j.1360-0443.1993.tb02761.x. PMID 8448514.
- ^ Driving Under the Influence: A Report to Congress on Alcohol Limits. U.S. Department of Transportation, National Highway Traffic Safety Administration. 1992. pp. 1–.
- ^ "Legislative History of .08 per se Laws – NHTSA". NHTSA. National Highway Traffic Safety Administration. July 2001. Retrieved 21 July 2017.
- ^ Nelson B. "Nevada's Driving Under the Influence (DUI) laws". NVPAC. Advisory Council for Prosecuting Attorneys. Archived from the original on 22 April 2017. Retrieved 3 July 2017.
- ^ "Application to Include Fomepizole on the WHO Model List of Essential Medicines" (PDF). November 2012. p. 10.
- ^ a b Vale A (2007). "Methanol". Medicine. 35 (12): 633–4. doi:10.1016/j.mpmed.2007.09.014.
- ^ "Methanol Poisoning Overview". Antizol. Archived from the original on 5 October 2011. Retrieved 11 October 2011. dead link
- ^ "Methanol (CASRN 67–56–1)". Integrated Risk Information System (IRIS). U.S. Environmental Protection Agency.
- ^ "Tourists drinks spiked with date rape drugs by thieving gangs in Benidorm". Metro. 19 June 2019.
- ^ "How to tell if your drink has been spiked on a night out and what to do". The Independent. 20 September 2018. Archived from the original on 14 May 2022.
- ^ Hall JA, Moore CB (July 2008). "Drug facilitated sexual assault—a review". Journal of Forensic and Legal Medicine. 15 (5): 291–7. doi:10.1016/j.jflm.2007.12.005. PMID 18511003.
- ^ Beynon CM, McVeigh C, McVeigh J, Leavey C, Bellis MA (July 2008). "The involvement of drugs and alcohol in drug-facilitated sexual assault: a systematic review of the evidence". Trauma, Violence & Abuse. 9 (3): 178–88. doi:10.1177/1524838008320221. PMID 18541699. S2CID 27520472.
- ^ "Alcohol Is Most Common 'Date Rape' Drug". Medicalnewstoday.com. Archived from the original on 17 October 2007. Retrieved 1 June 2011.
- ^ Schwartz RH, Milteer R, LeBeau MA (June 2000). "Drug-facilitated sexual assault ('date rape')". Southern Medical Journal. 93 (6): 558–61. doi:10.1097/00007611-200093060-00002. PMID 10881768.
- ^ a b Holstege CP, Saathoff GB, Neer TM, Furbee RB, eds. (25 October 2010). Criminal poisoning: clinical and forensic perspectives. Sudbury, Mass.: Jones and Bartlett Publishers. pp. 232. ISBN 978-0-7637-4463-2.
- ^ "Date Rape". Survive.org.uk. 20 March 2000. Retrieved 1 June 2011.
- ^ "Consumption of alcohol/energy drink mixes linked with casual, risky sex". ScienceDaily.
- ^ Ball NJ, Miller KE, Quigley BM, Eliseo-Arras RK (April 2021). "Alcohol Mixed With Energy Drinks and Sexually Related Causes of Conflict in the Barroom". Journal of Interpersonal Violence. 36 (7–8): 3353–3373. doi:10.1177/0886260518774298. PMID 29779427. S2CID 29150434.
- ^ Chersich MF, Rees HV (January 2010). "Causal links between binge drinking patterns, unsafe sex and HIV in South Africa: its time to intervene". International Journal of STD & AIDS. 21 (1): 2–7. doi:10.1258/ijsa.2000.009432. PMID 20029060. S2CID 3100905.
- ^ "England gets a taste for Buckfast, the fortified wine that's linked to crime". The Daily Telegraph. 17 July 2017.
- ^ "Alcohol-Related Crimes: Statistics and Facts". Alcohol Rehab Guide. Retrieved 3 September 2019.
- ^ "Alcohol statistics". Alcohol Change UK. Retrieved 22 September 2019.
- ^ Dingwall G (23 July 2013). Alcohol and Crime. Routledge. pp. 160–161. ISBN 978-1-134-02970-9.
- ^ Standridge JB, Zylstra RG, Adams SM (July 2004). "Alcohol consumption: an overview of benefits and risks". Southern Medical Journal. 97 (7): 664–672. doi:10.1097/00007611-200407000-00012. PMID 15301124. S2CID 26801239.
- ^ Kuntsche E, Rehm J, Gmel G (July 2004). "Characteristics of binge drinkers in Europe". Social Science & Medicine. 59 (1): 113–127. doi:10.1016/j.socscimed.2003.10.009. PMID 15087148.
- ^ Clark DB, Bukstein O, Cornelius J (2002). "Alcohol use disorders in adolescents: epidemiology, diagnosis, psychosocial interventions, and pharmacological treatment". Paediatric Drugs. 4 (8): 493–502. doi:10.2165/00128072-200204080-00002. PMID 12126453. S2CID 30900197.
- ^ Floyd RL, O'Connor MJ, Sokol RJ, Bertrand J, Cordero JF (November 2005). "Recognition and prevention of fetal alcohol syndrome". Obstetrics and Gynecology. 106 (5 Pt 1): 1059–1064. CiteSeerX 10.1.1.537.7292. doi:10.1097/01.AOG.0000181822.91205.6f. PMID 16260526.
- ^ Compare: Stolle M, Sack PM, Thomasius R (May 2009). "Binge drinking in childhood and adolescence: epidemiology, consequences, and interventions". Deutsches Arzteblatt International. 106 (19): 323–328. doi:10.3238/arztebl.2009.0323. PMC 2689602. PMID 19547732.
Excessive episodic consumption of alcohol is usually referred to these days as 'binge drinking.'
- ^ Trub L, Doyle KM, Parker V, Starks TJ (2021). "Drunk Texting: When the Phone Becomes a Vehicle for Emotional Dysregulation and Problematic Alcohol Use". Substance Use & Misuse. 56 (12): 1815–1824. doi:10.1080/10826084.2021.1954027. PMID 34353214.
- ^ Youssef NA, Rich CL (2008). "Does acute treatment with sedatives/hypnotics for anxiety in depressed patients affect suicide risk? A literature review". Annals of Clinical Psychiatry. 20 (3): 157–69. doi:10.1080/10401230802177698. PMID 18633742.
- ^ a b Vijayakumar L, Kumar MS, Vijayakumar V (May 2011). "Substance use and suicide". Current Opinion in Psychiatry. 24 (3): 197–202. doi:10.1097/YCO.0b013e3283459242. PMID 21430536. S2CID 206143129.
- ^ a b Sher L (January 2006). "Alcohol consumption and suicide". QJM. 99 (1): 57–61. doi:10.1093/qjmed/hci146. PMID 16287907.
- ^ Sher L (2007). "Functional magnetic resonance imaging in studies of the neurobiology of suicidal behavior in adolescents with alcohol use disorders". International Journal of Adolescent Medicine and Health. 19 (1): 11–18. doi:10.1515/ijamh.2007.19.1.11. PMID 17458319. S2CID 42672912.
- ^ a b c Yost DA (2002). "Acute care for alcohol intoxication" (PDF). Postgraduate Medicine Online. 112 (6). Archived from the original (PDF) on 14 December 2010. Retrieved 29 September 2007.
- ^ "Drunkest driver in SA arrested". SowetanLIVE. Retrieved 12 April 2024.
- ^ Iida-Ueno A, Enomoto M, Tamori A, Kawada N (April 2017). "Hepatitis B virus infection and alcohol consumption". World Journal of Gastroenterology. 23 (15): 2651–2659. doi:10.3748/wjg.v23.i15.2651. PMC 5403744. PMID 28487602.
- ^ Maintz L, Novak N (May 2007). "Histamine and histamine intolerance". The American Journal of Clinical Nutrition. 85 (5): 1185–1196. doi:10.1093/ajcn/85.5.1185. PMID 17490952.
- ^ D'Souza S, Mayock S, Salt A (December 2017). "A review of in vivo and in vitro aspects of alcohol-induced dose dumping". AAPS Open. 3 (1). doi:10.1186/s41120-017-0014-9. ISSN 2364-9534.
- ^ Lukas SE, Orozco S (October 2001). "Ethanol increases plasma Delta(9)-tetrahydrocannabinol (THC) levels and subjective effects after marihuana smoking in human volunteers". Drug and Alcohol Dependence. 64 (2): 143–9. doi:10.1016/S0376-8716(01)00118-1. PMID 11543984.
- ^ Repchinsky C (ed.) (2012). Compendium of pharmaceuticals and specialties, Ottawa: Canadian Pharmacists Association.[full citation needed]
- ^ "Alcohol & Diabetes – ADA". American Diabetes Association. Retrieved 30 November 2022.
- ^ Agrawal N (June 1991). "Risk factors for gastrointestinal ulcers caused by nonsteroidal anti-inflammatory drugs (NSAIDs)". The Journal of Family Practice. 32 (6): 619–624. PMID 2040888.
- ^ Laizure SC, Mandrell T, Gades NM, Parker RB (January 2003). "Cocaethylene metabolism and interaction with cocaine and ethanol: role of carboxylesterases". Drug Metabolism and Disposition. 31 (1): 16–20. doi:10.1124/dmd.31.1.16. PMID 12485948.
- ^ Pergolizzi J, Breve F, Magnusson P, LeQuang JA, Varrassi G (February 2022). "Cocaethylene: When Cocaine and Alcohol Are Taken Together". Cureus. 14 (2): e22498. doi:10.7759/cureus.22498. PMC 8956485. PMID 35345678.
- ^ Markowitz JS, Logan BK, Diamond F, Patrick KS (August 1999). "Detection of the novel metabolite ethylphenidate after methylphenidate overdose with alcohol coingestion". Journal of Clinical Psychopharmacology. 19 (4): 362–6. doi:10.1097/00004714-199908000-00013. PMID 10440465.
- ^ Markowitz JS, DeVane CL, Boulton DW, Nahas Z, Risch SC, Diamond F, et al. (June 2000). "Ethylphenidate formation in human subjects after the administration of a single dose of methylphenidate and ethanol". Drug Metabolism and Disposition. 28 (6): 620–4. PMID 10820132.
- ^ Verplaetse TL, McKee SA (March 2017). "An overview of alcohol and tobacco/nicotine interactions in the human laboratory". The American Journal of Drug and Alcohol Abuse. 43 (2): 186–196. doi:10.1080/00952990.2016.1189927. PMC 5588903. PMID 27439453.
- ^ McCoy HG, Cipolle RJ, Ehlers SM, Sawchuk RJ, Zaske DE (November 1979). "Severe methanol poisoning. Application of a pharmacokinetic model for ethanol therapy and hemodialysis". The American Journal of Medicine. 67 (5): 804–7. doi:10.1016/0002-9343(79)90766-6. PMID 507092.
- ^ Weathermon R, Crabb DW (1999). "Alcohol and medication interactions". Alcohol Research & Health. 23 (1): 40–54. PMC 6761694. PMID 10890797.
- ^ "PRODUCT INFORMATION COUMADIN" (PDF). TGA eBusiness Services. Aspen Pharma Pty Ltd. 19 January 2010. Archived from the original on 17 October 2015. Retrieved 11 December 2013.
- ^ "Warfarin Anticoagulant Medication". Archived from the original on 1 July 2020. Retrieved 30 June 2020.
- ^ "Isoniazid tablet". DailyMed. 18 October 2018. Archived from the original on 13 March 2019. Retrieved 24 January 2020.
- ^ Saukkonen JJ, Cohn DL, Jasmer RM, Schenker S, Jereb JA, Nolan CM, et al. (October 2006). "An official ATS statement: hepatotoxicity of antituberculosis therapy". American Journal of Respiratory and Critical Care Medicine. 174 (8): 935–952. doi:10.1164/rccm.200510-1666ST. PMID 17021358. S2CID 36384722.
- ^ a b c d e f g h i j k l m n o p q r s Santhakumar V, Wallner M, Otis TS (May 2007). "Ethanol acts directly on extrasynaptic subtypes of GABAA receptors to increase tonic inhibition". Alcohol. 41 (3): 211–21. doi:10.1016/j.alcohol.2007.04.011. PMC 2040048. PMID 17591544.
- ^ a b c d e Spanagel R (April 2009). "Alcoholism: a systems approach from molecular physiology to addictive behavior". Physiological Reviews. 89 (2): 649–705. doi:10.1152/physrev.00013.2008. PMID 19342616.
- ^ a b c Söderpalm B, Lidö HH, Ericson M (November 2017). "The Glycine Receptor-A Functionally Important Primary Brain Target of Ethanol". Alcoholism: Clinical and Experimental Research. 41 (11): 1816–1830. doi:10.1111/acer.13483. PMID 28833225.
- ^ a b Wu J, Gao M, Taylor DH (March 2014). "Neuronal nicotinic acetylcholine receptors are important targets for alcohol reward and dependence". Acta Pharmacologica Sinica. 35 (3): 311–15. doi:10.1038/aps.2013.181. PMC 4647894. PMID 24464050.
- ^ Dopico AM, Bukiya AN, Kuntamallappanavar G, Liu J (2016). "Modulation of BK Channels by Ethanol". International Review of Neurobiology. 128: 239–79. doi:10.1016/bs.irn.2016.03.019. ISBN 978-0-12-803619-8. PMC 5257281. PMID 27238266.
- ^ a b c d e Möykkynen T, Korpi ER (July 2012). "Acute effects of ethanol on glutamate receptors". Basic & Clinical Pharmacology & Toxicology. 111 (1): 4–13. doi:10.1111/j.1742-7843.2012.00879.x. PMID 22429661.
- ^ a b c d Wallner M, Olsen RW (May 2008). "Physiology and pharmacology of alcohol: the imidazobenzodiazepine alcohol antagonist site on subtypes of GABAA receptors as an opportunity for drug development?". British Journal of Pharmacology. 154 (2): 288–98. doi:10.1038/bjp.2008.32. PMC 2442438. PMID 18278063.
- ^ a b c d e f g h Harrison NL, Skelly MJ, Grosserode EK, Lowes DC, Zeric T, Phister S, et al. (August 2017). "Effects of acute alcohol on excitability in the CNS". Neuropharmacology. 122: 36–45. doi:10.1016/j.neuropharm.2017.04.007. PMC 5657304. PMID 28479395.
- ^ Förstera B, Castro PA, Moraga-Cid G, Aguayo LG (2016). "Potentiation of Gamma Aminobutyric Acid Receptors (GABAAR) by Ethanol: How Are Inhibitory Receptors Affected?". Frontiers in Cellular Neuroscience. 10: 114. doi:10.3389/fncel.2016.00114. PMC 4858537. PMID 27199667.
- ^ Chung HW, Petersen EN, Cabanos C, Murphy KR, Pavel MA, Hansen AS, et al. (January 2019). "A Molecular Target for an Alcohol Chain-Length Cutoff". Journal of Molecular Biology. 431 (2): 196–209. doi:10.1016/j.jmb.2018.11.028. PMC 6360937. PMID 30529033.
- ^ Laverty D, Desai R, Uchański T, Masiulis S, Stec WJ, Malinauskas T, et al. (January 2019). "Cryo-EM structure of the human α1β3γ2 GABAA receptor in a lipid bilayer". Nature. 565 (7740): 516–20. Bibcode:2019Natur.565..516L. doi:10.1038/s41586-018-0833-4. PMC 6364807. PMID 30602789.
- ^ Cueva JP, Giorgioni G, Grubbs RA, Chemel BR, Watts VJ, Nichols DE (November 2006). "trans-2,3-dihydroxy-6a,7,8,12b-tetrahydro-6H-chromeno[3,4-c]isoquinoline: synthesis, resolution, and preliminary pharmacological characterization of a new dopamine D1 receptor full agonist". Journal of Medicinal Chemistry. 49 (23): 6848–6857. doi:10.1021/jm0604979. PMID 17154515.
- ^ Michaelides MR, Hong Y, DiDomenico S, Asin KE, Britton DR, Lin CW, et al. (September 1995). "(5aR,11bS)-4,5,5a,6,7,11b-hexahydro-2-propyl-3-thia-5-azacyclopent-1- ena[c]-phenanthrene-9,10-diol (A-86929): a potent and selective dopamine D1 agonist that maintains behavioral efficacy following repeated administration and characterization of its diacetyl prodrug (ABT-431)". Journal of Medicinal Chemistry. 38 (18): 3445–3447. doi:10.1021/jm00018a002. PMID 7658429.
- ^ Karahanian E, Quintanilla ME, Tampier L, Rivera-Meza M, Bustamante D, Gonzalez-Lira V, et al. (April 2011). "Ethanol as a prodrug: brain metabolism of ethanol mediates its reinforcing effects". Alcoholism: Clinical and Experimental Research. 35 (4): 606–12. doi:10.1111/j.1530-0277.2011.01439.x. PMC 3142559. PMID 21332529.
- ^ a b Melis M, Enrico P, Peana AT, Diana M (November 2007). "Acetaldehyde mediates alcohol activation of the mesolimbic dopamine system". The European Journal of Neuroscience. 26 (10): 2824–33. doi:10.1111/j.1460-9568.2007.05887.x. PMID 18001279. S2CID 25110014.
- ^ a b c d e "Alcoholism – Homo sapiens (human) Database entry". KEGG Pathway. 29 October 2014. Retrieved 9 February 2015.
- ^ a b c d e f g h Kanehisa Laboratories (29 October 2014). "Alcoholism – Homo sapiens (human)". KEGG Pathway. Retrieved 31 October 2014.
- ^ a b c d e Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. p. 372. ISBN 978-0-07-148127-4.
- ^ Ruffle JK (November 2014). "Molecular neurobiology of addiction: what's all the (Δ)FosB about?". The American Journal of Drug and Alcohol Abuse. 40 (6): 428–37. doi:10.3109/00952990.2014.933840. PMID 25083822. S2CID 19157711.
- ^ Nestler EJ (December 2013). "Cellular basis of memory for addiction". Dialogues in Clinical Neuroscience. 15 (4): 431–43. doi:10.31887/DCNS.2013.15.4/enestler. PMC 3898681. PMID 24459410.
Despite the Importance of Numerous Psychosocial Factors, at its Core, Drug Addiction Involves a Biological Process: the ability of repeated exposure to a drug of abuse to induce changes in a vulnerable brain that drive the compulsive seeking and taking of drugs, and loss of control over drug use, that define a state of addiction. ... A large body of literature has demonstrated that such ΔFosB induction in D1-type NAc neurons increases an animal's sensitivity to drug as well as natural rewards and promotes drug self-administration, presumably through a process of positive reinforcement
- ^ Robison AJ, Nestler EJ (October 2011). "Transcriptional and epigenetic mechanisms of addiction". Nature Reviews. Neuroscience. 12 (11): 623–37. doi:10.1038/nrn3111. PMC 3272277. PMID 21989194.
- ^ Pohorecky LA, Brick J (1988). "Pharmacology of ethanol". Pharmacology & Therapeutics. 36 (2–3): 335–427. doi:10.1016/0163-7258(88)90109-X. PMID 3279433.
- ^ a b Liu Y, Hunt WA (6 December 2012). The "Drunken" Synapse: Studies of Alcohol-Related Disorders. Springer Science & Business Media. pp. 40–. ISBN 978-1-4615-4739-6.
- ^ Rubin R, Strayer DS, Rubin E, McDonald JM (2008). Rubin's Pathology: Clinicopathologic Foundations of Medicine. Lippincott Williams & Wilkins. pp. 257–. ISBN 978-0-7817-9516-6.
- ^ Situmorang JH, Lin HH, Lo H, Lai CC (January 2018). "Role of neuronal nitric oxide synthase (nNOS) at medulla in tachycardia induced by repeated administration of ethanol in conscious rats". Journal of Biomedical Science. 25 (1): 8. doi:10.1186/s12929-018-0409-5. PMC 5791364. PMID 29382335.
- ^ Steffensen SC, Shin SI, Nelson AC, Pistorius SS, Williams SB, Woodward TJ, et al. (September 2017). "α6 subunit-containing nicotinic receptors mediate low-dose ethanol effects on ventral tegmental area neurons and ethanol reward". Addiction Biology. 23 (5): 1079–1093. doi:10.1111/adb.12559. PMC 5849490. PMID 28901722.
- ^ Sitte H, Freissmuth M (2 August 2006). Neurotransmitter Transporters. Springer Science & Business Media. pp. 472–. ISBN 978-3-540-29784-0.
- ^ Allen-Gipson DS, Jarrell JC, Bailey KL, Robinson JE, Kharbanda KK, Sisson JH, et al. (May 2009). "Ethanol blocks adenosine uptake via inhibiting the nucleoside transport system in bronchial epithelial cells". Alcoholism: Clinical and Experimental Research. 33 (5): 791–98. doi:10.1111/j.1530-0277.2009.00897.x. PMC 2940831. PMID 19298329.
- ^ a b c d e Henri B, Kissin B (1996). The Pharmacology of Alcohol and Alcohol Dependence. Oxford University Press. pp. 18–. ISBN 978-0-19-510094-5.
- ^ Mitchell MC, Teigen EL, Ramchandani VA (May 2014). "Absorption and peak blood alcohol concentration after drinking beer, wine, or spirits". Alcoholism: Clinical and Experimental Research. 38 (5): 1200–1204. doi:10.1111/acer.12355. PMC 4112772. PMID 24655007.
- ^ "Champagne does get you drunk faster". New Scientist.
- ^ a b Agarwal DP, Goedde HW (April 1992). "Pharmacogenetics of alcohol metabolism and alcoholism". Pharmacogenetics. 2 (2): 48–62. doi:10.1097/00008571-199204000-00002. PMID 1302043.
- ^ Lansdorp B, Ramsay W, Hamidand R, Strenk E (May 2019). "Wearable Enzymatic Alcohol Biosensor". Sensors. 19 (10): 2380. Bibcode:2019Senso..19.2380L. doi:10.3390/s19102380. PMC 6566815. PMID 31137611.
- ^ "SCRAM CAM® Bracelet Alcohol Ankle Monitor". SCRAM Systems. Retrieved 19 March 2022.
- ^ "ION Wearable". ION Wearable. Retrieved 19 March 2022.
- ^ "Distillation: Some Purity Considerations". Moonshine Still. Retrieved 5 May 2015.
- ^ Blumenthal P, Steger MC, Einfalt D, Rieke-Zapp J, Quintanilla Bellucci A, Sommerfeld K, et al. (April 2021). "Methanol Mitigation during Manufacturing of Fruit Spirits with Special Consideration of Novel Coffee Cherry Spirits". Molecules. 26 (9): 2585. doi:10.3390/molecules26092585. PMC 8125215. PMID 33925245.
- ^ Hui-Ling Ma, Xiu-Ping Yang, Ying Zuo (15 April 2006). "Study on Method of Decreasing Methanol in Apple Pomace Spirit". Food Science. 27 (4): 138–142.
- ^ a b c d Philp RB (15 September 2015). Ecosystems and Human Health: Toxicology and Environmental Hazards (Third ed.). CRC Press. pp. 216–. ISBN 978-1-4987-6008-9.
- ^ n-Butanol (PDF), SIDS Initial Assessment Report, Geneva: United Nations Environment Programme, April 2005.
- ^ McCreery MJ, Hunt WA (July 1978). "Physico-chemical correlates of alcohol intoxication". Neuropharmacology. 17 (7): 451–61. doi:10.1016/0028-3908(78)90050-3. PMID 567755. S2CID 19914287.
- ^ Carey F (2000). Organic Chemistry (4th ed.). McGraw-Hill. ISBN 0-07-290501-8. Retrieved 5 February 2013.
- ^ Glauser FL, Smith WR, Caldwell A, Hoshiko M, Dolan GS, Baer H, et al. (January 1976). "Ethchlorvynol (Placidyl)-induced pulmonary edema". Annals of Internal Medicine. 84 (1): 46–48. doi:10.7326/0003-4819-84-1-46. PMID 942681.
- ^ Carr T, Kilian C, Llamosas-Falcón L, Zhu Y, Lasserre AM, Puka K, et al. (March 2024). "The risk relationships between alcohol consumption, alcohol use disorder and alcohol use disorder mortality: A systematic review and meta-analysis". Addiction (preprint): 1–14. doi:10.1111/add.16456. PMID 38450868.
- ^ Babor T, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, et al. (2010). Alcohol: No Ordinary Commodity: Research and Public Policy (2nd ed.). Oxford: Oxford University Press. ISBN 978-0-19-955114-9. OCLC 656362316.
- ^ a b Dunbar RI, Launay J, Wlodarski R, Robertson C, Pearce E, Carney J, et al. (June 2017). "Functional Benefits of (Modest) Alcohol Consumption". Adaptive Human Behavior and Physiology. 3 (2): 118–33. doi:10.1007/s40750-016-0058-4. PMC 7010365. PMID 32104646.
- ^ Sayette MA, Creswell KG, Dimoff JD, Fairbairn CE, Cohn JF, Heckman BW, et al. (August 2012). "Alcohol and group formation: a multimodal investigation of the effects of alcohol on emotion and social bonding". Psychological Science. 23 (8): 869–78. doi:10.1177/0956797611435134. PMC 5462438. PMID 22760882.
- ^ Ruthven M (1997). Islam: a very short introduction. New York: Oxford University Press. ISBN 978-0-19-154011-0. OCLC 43476241.
- ^ Gentry K (2001). God Gave Wine. Oakdown. pp. 3ff. ISBN 0-9700326-6-8.
- ^ Talmud Megillah 7b
- ^ Borras L, Khazaal Y, Khan R, Mohr S, Kaufmann YA, Zullino D, et al. (December 2010). "The relationship between addiction and religion and its possible implication for care". Substance Use & Misuse. 45 (14): 2357–2410. doi:10.3109/10826081003747611. PMC 4137975. PMID 21039108.
- ^ "Drinking on Purim". aishcom. 28 February 2015.
- ^ a b c d e Boyle P (7 March 2013). Alcohol: Science, Policy and Public Health. OUP Oxford. pp. 363–. ISBN 978-0-19-965578-6.
- ^ "Getting a drink in Saudi Arabia". BBC News. BBC. 8 February 2001. Retrieved 7 July 2015.
- ^ "Can you drink alcohol in Saudi Arabia?". 1 August 2012. Retrieved 7 July 2015.
- ^ "13 Countries With Booze Bans". Swifty.com. Archived from the original on 2 July 2015. Retrieved 7 July 2015.
- ^ "Two Iranians Sentenced to Death for Drinking Alcohol, AFP Says - Businessweek". Archived from the original on 28 June 2012. Retrieved 25 June 2012.
- ^ "Iran to execute two for alcohol: Reports". Archived from the original on 25 June 2012. Retrieved 25 June 2012.
- ^ Zhao J, Stockwell T, Vallance K, Hobin E (March 2020). "The Effects of Alcohol Warning Labels on Population Alcohol Consumption: An Interrupted Time Series Analysis of Alcohol Sales in Yukon, Canada". Journal of Studies on Alcohol and Drugs. 81 (2): 225–37. doi:10.15288/jsad.2020.81.225. PMID 32359054. S2CID 218481829.
- ^ "Alcohol labelling: A discussion document on policy options" (PDF). World Health Organization.
- ^ a b "2019 AICR Cancer Risk Awareness Survey" (PDF). AICR 2019 Cancer Risk Awareness Survey. 2019.
- ^ Greene NK, Rising CJ, Seidenberg AB, Eck R, Trivedi N, Oh AY (May 2023). "Exploring correlates of support for restricting breast cancer awareness marketing on alcohol containers among women". The International Journal on Drug Policy. 115: 104016. doi:10.1016/j.drugpo.2023.104016. PMC 10593197. PMID 36990013.
- ^ Atkinson AM, Meadows BR, Sumnall H (February 2024). "'Just a colour?': Exploring women's relationship with pink alcohol brand marketing within their feminine identity making". The International Journal on Drug Policy. 125: 104337. doi:10.1016/j.drugpo.2024.104337. PMID 38335868.
- ^ Hall MG, Lee CJ, Jernigan DH, Ruggles P, Cox M, Whitesell C, et al. (May 2024). "The impact of "pinkwashed" alcohol advertisements on attitudes and beliefs: A randomized experiment with US adults". Addictive Behaviors. 152: 107960. doi:10.1016/j.addbeh.2024.107960. PMC 10923020. PMID 38309239.
- ^ Mart S, Giesbrecht N (October 2015). "Red flags on pinkwashed drinks: contradictions and dangers in marketing alcohol to prevent cancer". Addiction. 110 (10): 1541–1548. doi:10.1111/add.13035. PMID 26350708.
- ^ Spivey JD, Lee JG, Smallwood SW (February 2018). "Tobacco Policies and Alcohol Sponsorship at Lesbian, Gay, Bisexual, and Transgender Pride Festivals: Time for Intervention". American Journal of Public Health. 108 (2): 187–188. doi:10.2105/AJPH.2017.304205. PMC 5846596. PMID 29320286.
- ^ "AUDIT The Alcohol Use Disorders Identification Test" (pdf). WHO (2nd ed.). 2001. Retrieved 2 January 2020.
- ^ Kalinowski A, Humphreys K (July 2016). "Governmental standard drink definitions and low-risk alcohol consumption guidelines in 37 countries". Addiction. 111 (7): 1293–1298. doi:10.1111/add.13341. PMID 27073140.
- ^ Results from the 2013 National Survey on Drug Use and Health: Summary of National Findings (PDF) (Report). NSDUH Series H-48. Rockville, MD: Substance Abuse and Mental Health Services Administration. September 2014. HHS Publication No. (SMA) 14-4863. Retrieved 11 June 2015.
- ^ Goddiksen MK (4 January 2023). "Sober Curious er det nye sort'" [Sober Curious is the new kind] (in Danish).
- ^ What Does It Mean to Be Sober Curious? article by Sarah Sheppard, January 24, 2021, on verywellmind
- ^ Skål – uden alkohol, article by Eva Guld Boesen in Samvirke ISSN 0036-3944, February 2023, pp. 18-27 (in Danish)
- ^ Kilian C, O'Donnell A, Potapova N, López-Pelayo H, Schulte B, Miquel L, et al. (May 2022). "Changes in alcohol use during the COVID-19 pandemic in Europe: A meta-analysis of observational studies". Drug and Alcohol Review. 41 (4): 918–931. doi:10.1111/dar.13446. PMC 9111882. PMID 35187739.
- ^ "History of Alcohol" (PDF). Archived from the original (PDF) on 21 August 2013. Retrieved 11 May 2015.
- ^ "Motbok" [Counter book]. Förvaltningshistorisk ordbok [Administrative history dictionary] (in Swedish). Retrieved 3 November 2022.
- ^ "Alkoholikeeldudest Eestis". Postimees (in Estonian). 8 November 2008. Retrieved 27 March 2024.
Further reading edit
- The National Institute on Alcohol Abuse and Alcoholism maintains a database of alcohol-related health effects. ETOH Archival Database (1972–2003) Alcohol and Alcohol Problems Science Database.
External links edit
- WHO fact sheet on alcohol
- ChEBI – biology related
- Kyoto Encyclopedia of Genes and Genomes signal transduction pathway: KEGG – human alcohol addiction
- Benton SA. "The High-Functioning Alcoholic". Psychology Today.