


Summary
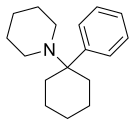
Phencyclidine or phenylcyclohexyl piperidine (PCP), also known in its use as a street drug as angel dust among other names, is a dissociative anesthetic mainly used recreationally for its significant mind-altering effects.[1][5] PCP may cause hallucinations, distorted perceptions of sounds, and violent behavior.[5][8][9] As a recreational drug, it is typically smoked, but may be taken by mouth, snorted, or injected.[5][6][8] It may also be mixed with cannabis or tobacco.[1][5]
 | |
 | |
| Clinical data | |
|---|---|
| Trade names | Sernyl, Sernylan (both discontinued) |
| Other names | CI-395; Phenylcyclohexylpiperidine; "Angel dust"[1] |
| AHFS/Drugs.com | phencyclidine |
| Dependence liability | Physical: Low Psychological: Moderate[2] |
| Addiction liability | Variable, reported from low to high[3][4] |
| Routes of administration | Smoking, injection, snorted, by mouth[5][6] |
| Drug class | NMDA receptor antagonists; General anesthetics; Dissociative hallucinogens[5] |
| ATC code |
|
| Legal status | |
| Legal status |
|
| Pharmacokinetic data | |
| Metabolism | Oxidative hydroxylation in liver by CYP450 enzymes, glucuronidation |
| Metabolites | PCHP, PPC, PCAA |
| Onset of action | 2–60 min[7] |
| Elimination half-life | 7–46 hours |
| Duration of action | 6–48 hours[7] |
| Excretion | Urine |
| Identifiers | |
| |
| CAS Number |
|
| PubChem CID |
|
| IUPHAR/BPS |
|
| DrugBank |
|
| ChemSpider |
|
| UNII |
|
| KEGG |
|
| ChEBI |
|
| ChEMBL |
|
| CompTox Dashboard (EPA) |
|
| ECHA InfoCard | 100.150.427 |
| Chemical and physical data | |
| Formula | C17H25N |
| Molar mass | 243.394 g·mol−1 |
| 3D model (JSmol) |
|
| Melting point | 46.5 °C (115.7 °F) |
| Boiling point | 136 °C (277 °F) |
| |
| |
| Data page | |
| Phencyclidine (data page) | |
| | |
Adverse effects may include seizures, coma, addiction, and an increased risk of suicide.[8] Flashbacks may occur despite stopping usage.[9] Chemically, PCP is a member of the arylcyclohexylamine class, and pharmacologically, it is a dissociative anesthetic.[5][10][11] PCP works primarily as an NMDA receptor antagonist.[10]
PCP is most commonly used in the United States.[12] While usage peaked in the US in the 1970s,[13] between 2005 and 2011 an increase in visits to emergency departments as a result of the drug occurred.[8] As of 2017 in the United States, about 1% of people in 12th grade reported using PCP in the prior year while 2.9% of those over the age of 25 reported using it at some point in their lives.[14]
Recreational uses edit

Phencyclidine is used for its ability to induce a dissociative state.[15]
Effects edit
Behavioral effects can vary by dosage. Low doses produce a numbness in the extremities and intoxication, characterized by staggering, unsteady gait, slurred speech, bloodshot eyes, and loss of balance. Moderate doses (5–10 mg intranasal, or 0.01–0.02 mg/kg intramuscular or intravenous) will produce analgesia and anesthesia. High doses may lead to convulsions.[16] The drug is often illegally produced under poorly controlled conditions; this means that users may be unaware of the actual dose they are taking.[17]
Psychological effects include severe changes in body image, loss of ego boundaries, paranoia, and depersonalization. Psychosis, agitation and dysphoria, hallucinations, blurred vision, euphoria, and suicidal impulses are also reported, as well as occasional aggressive behavior.[18][19]: 48–49 [16] Like many other drugs, PCP has been known to alter mood states in an unpredictable fashion, causing some individuals to become detached, and others to become animated. PCP may induce feelings of strength, power, and invulnerability as well as a numbing effect on the mind.[6]
Studies by the Drug Abuse Warning Network in the 1970s show that media reports of PCP-induced violence are greatly exaggerated and that incidents of violence are unusual and often limited to individuals with reputations for aggression regardless of drug use.[19]: 48 Although uncommon, events of PCP-intoxicated individuals acting in an unpredictable fashion, possibly driven by their delusions or hallucinations, have been publicized.[20] Other commonly cited types of incidents include inflicting property damage and self-mutilation of various types, such as pulling one's own teeth.[19]: 48 [20] These effects were not noted in its medicinal use in the 1950s and 1960s, however, and reports of physical violence on PCP have often been shown to be unfounded.[21][22]
Recreational doses of the drug also occasionally appear to induce a psychotic state, with emotional and cognitive impairment that resembles a schizophrenic episode.[23][24] Users generally report feeling detached from reality.[25]
Symptoms are summarized by the mnemonic device RED DANES: rage, erythema (redness of skin), dilated pupils, delusions, amnesia, nystagmus (oscillation of the eyeball when moving laterally), excitation, and skin dryness.[26]
Addiction edit
PCP is self-administered and induces ΔFosB expression in the D1-type medium spiny neurons of the nucleus accumbens,[3][27] and accordingly, excessive PCP use is known to cause addiction.[3] PCP's rewarding and reinforcing effects are at least partly mediated by blocking the NMDA receptors in the glutamatergic inputs to D1-type medium spiny neurons in the nucleus accumbens.[3] PCP has been shown to produce conditioned place aversion and conditioned place preference in animal studies.[28]
Schizophrenia edit
A 2019 review found that the transition rate from a diagnosis of hallucinogen-induced psychosis (which included PCP) to that of schizophrenia was 26%. This was lower than cannabis-induced psychosis (34%) but higher than amphetamine (22%), opioid (12%), alcohol (10%), and sedative (9%) induced psychoses. In comparison, the transition rate to schizophrenia for "brief, atypical and not otherwise specified" psychosis was found to be 36%.[29]
Methods of administration edit
PCP is easily accessible because of the various routes of administration available. Most commonly, the powder form of the drug is snorted. PCP can also be orally ingested, injected subcutaneously or intravenously, or smoked laced with marijuana or cigarettes.[30]
- PCP can be ingested through smoking. "Fry" and "sherm" are street terms for marijuana or tobacco cigarettes that are dipped in PCP and then dried.[31]
- PCP hydrochloride can be insufflated (snorted), depending upon the purity. This is most often referred to as "angel dust".[30]
- An oral pill can also be compressed from the co-compounded powder form of the drug. This is usually referred to as "peace pill".[30]
- The free base is hydrophobic and may be absorbed through skin and mucus membranes (often inadvertently). This form of the drug is commonly called "wack".[30]
Management of intoxication edit
Management of PCP intoxication mostly consists of supportive care – controlling breathing, circulation, and body temperature – and, in the early stages, treating psychiatric symptoms.[32][33][34] Benzodiazepines, such as lorazepam, are the drugs of choice to control agitation and seizures (when present). Typical antipsychotics such as phenothiazines and haloperidol have been used to control psychotic symptoms, but may produce many undesirable side effects – such as dystonia – and their use is therefore no longer preferred; phenothiazines are particularly risky, as they may lower the seizure threshold, worsen hyperthermia, and boost the anticholinergic effects of PCP.[32][33] If an antipsychotic is given, intramuscular haloperidol has been recommended.[34][35][36]
Forced acid diuresis (with ammonium chloride or, more safely, ascorbic acid) may increase clearance of PCP from the body, and was somewhat controversially recommended in the past as a decontamination measure.[32][33][34] However, it is now known that only around 10% of a dose of PCP is removed by the kidneys, which would make increased urinary clearance of little consequence; furthermore, urinary acidification is dangerous, as it may induce acidosis and worsen rhabdomyolysis (muscle breakdown), a not-unusual manifestation of PCP toxicity.[32][33]
Pharmacology edit
Pharmacodynamics edit
| Site | Ki (nM) | Action | Species | Ref |
|---|---|---|---|---|
| NMDA | 44–59 | Antagonist | Human | [39][40] |
| MOR | >10,000 | ND | Human | [39] |
| DOR | >10,000 | ND | Human | [39] |
| KOR | >10,000 | ND | Human | [39] |
| NOP | >10,000 | ND | Human | [39] |
| σ1 | >10,000 | Agonist | Guinea pig | [39][41] |
| σ2 | 136 | Agonist | Rat | [39] |
| D2 | >10,000 | ND | Human | [39] |
| D2High | 2.7–4.3 144 (EC50) |
Partial Agonist | Rat/human Human |
[42][43] [44] |
| 5-HT2A | >10,000 | ND | Human | [39] |
| 5-HT2AHigh | ≥5,000 | Agonist? | Rat | [43][45] |
| SERT | 2,234 | Inhibitor | Human | [39] |
| NET | >10,000 | Inhibitor | Human | [39] |
| DAT | >10,000 | Inhibitor | Human | [39] |
| PCP2 | 154 | ND | Human | [40] |
| [3H]5-HT uptake | 1,424 (IC50) | Inhibitor | Rat | [46] |
| [3H]NIS binding | 16,628 (IC50) | Inhibitor | Rat | [46] |
| [3H]DA uptake | 347 (IC50) | Inhibitor | Rat | [46] |
| [3H]CFT binding | 1,547 (IC50) | Inhibitor | Rat | [46] |
| Values are Ki (nM). The smaller the value, the more strongly the drug binds to the site. | ||||
PCP is well known for its primary action on the NMDA receptor, an ionotropic glutamate receptor.[47][44] As such, PCP is a noncompetitive NMDA receptor antagonist. The role of NMDAR antagonism in the effect of PCP, ketamine, and related dissociative agents was first published in the early 1980s by David Lodge[48] and colleagues.[49] Other NMDA receptor antagonists include ketamine,[50] tiletamine,[51] dextromethorphan,[52] nitrous oxide, and dizocilpine (MK-801).
Research also indicates that PCP inhibits nicotinic acetylcholine receptors (nAChRs) among other mechanisms. Analogues of PCP exhibit varying potency at nACh receptors[53] and NMDA receptors.[54] Findings demonstrate that presynaptic nAChRs and NMDA receptor interactions influence postsynaptic maturation of glutamatergic synapses and consequently impact synaptic development and plasticity in the brain.[55] These effects can lead to inhibition of excitatory glutamate activity in certain brain regions such as the hippocampus[56] and cerebellum[57] thus potentially leading to memory loss as one of the effects of prolonged use. Acute effects on the cerebellum manifest as changes in blood pressure, breathing rate, pulse rate, and loss of muscular coordination during intoxication.[9]
PCP, like ketamine, also acts as a potent dopamine D2High receptor partial agonist in rat brain homogenate[44] and has affinity for the human cloned D2High receptor.[58] This activity may be associated with some of the other more psychotic features of PCP intoxication, which is evidenced by the successful use of D2 receptor antagonists (such as haloperidol) in the treatment of PCP psychosis.[59]
In addition to its well explored interactions with NMDA receptors, PCP has also been shown to inhibit dopamine reuptake, and thereby leads to increased extracellular levels of dopamine and hence increased dopaminergic neurotransmission.[60] However, PCP has little affinity for the human monoamine transporters, including the dopamine transporter (DAT).[39] Instead, its inhibition of monoamine reuptake may be mediated by interactions with allosteric sites on the monoamine transporters.[39] PCP is notably a high-affinity ligand of the PCP site 2 (Ki = 154 nM), a not-well-characterized site associated with monoamine reuptake inhibition.[40]
Studies on rats indicate that PCP interacts indirectly with opioid receptors (endorphin and enkephalin) to produce analgesia.[61]
A binding study assessed PCP at 56 sites including neurotransmitter receptors and transporters and found that PCP had Ki values of >10,000 nM at all sites except the dizocilpine (MK-801) site of the NMDA receptor (Ki = 59 nM), the σ2 receptor (PC12) (Ki = 136 nM), and the serotonin transporter (Ki = 2,234 nM).[39] The study notably found Ki values of >10,000 nM for the D2 receptor, the opioid receptors, the σ1 receptor, and the dopamine and norepinephrine transporters.[39] These results suggest that PCP is a highly selective ligand of the NMDAR and σ2 receptor.[39] However, PCP may also interact with allosteric sites on the monoamine transporters to produce inhibition of monoamine reuptake.[39]
Mechanism of action edit
Phencyclidine is a noncompetitive NMDA receptor antagonist that blocks the activity of the NMDA receptor to cause anaesthesia and analgesia without causing cardiorespiratory depression.[62][18] NMDA is an excitatory receptor in the brain, when activated normally the receptor acts as an ion channel and there is an influx of positive ions through the channel to cause nerve cell depolarisation. Phencyclidine inhibits the NMDA receptor by binding to the specific PCP binding site located within the ion channel.[63] The PCP binding site is within close proximity to the magnesium blocking site, which may explain the similar inhibitory effects.[64] Binding at the PCP site is mediated by two non-covalent interactions within the receptor: hydrogen bonding and hydrophobic interaction.[65] Binding is also controlled by the gating mechanism of the ion channel. Because the PCP site is located within the ion channel, a coagonist such as glycine must bind and open the channel in order for PCP to enter, bind to the PCP site, and block the channel.[66]
Neurotoxicity edit
Some studies found that, like other NMDA receptor antagonists, PCP can cause a kind of brain damage called Olney's lesions in rats.[67][68] Studies conducted on rats showed that high doses of the NMDA receptor antagonist dizocilpine caused reversible vacuoles to form in certain regions of the rats' brains. All studies of Olney's lesions have only been performed on non-human animals and may not apply to humans. One unpublished study by Frank Sharp reportedly showed no damage by the NDMA antagonist ketamine, a structurally similar drug, far beyond recreational doses,[69] but due to the study never having been published, its validity is controversial.
PCP has also been shown to cause schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate levels in the rat brain, which are detectable both in living rats and upon necropsy examination of brain tissue.[70] It also induces symptoms in humans that mimic schizophrenia.[71] PCP not only produced symptoms similar to schizophrenia, it also yielded electroencephalogram changes in the thalamocortical pathway (increased delta decreased alpha) and in the hippocampus (increase theta bursts) that were similar to those in schizophrenia.[72] PCP-induced augmentation of dopamine release may link the NMDA and dopamine hypotheses of schizophrenia.[73]
Pharmacokinetics edit

PCP is both water and lipid soluble and is therefore distributed throughout the body quickly.[64] PCP is metabolized into PCHP, PPC and PCAA. The drug is metabolized 90% by oxidative hydroxylation in the liver during the first pass. Metabolites are glucuronidated and excreted in the urine. Nine percent of ingested PCP is excreted in its unchanged form.[18]
When smoked, some of the compound is broken down by heat into 1-phenylcyclohexene (PC) and piperidine.
The time taken before the effects of PCP manifest is dependent on the route of administration. The onset of action for inhalation occurs in 2–5 minutes, whereas the effects may take 15 to 60 minutes when ingested orally.[18]
Chemistry edit
PCP is an arylcyclohexylamine.
Analogues edit

Fewer than 30 different analogs of PCP were reported as being used as a street drug during the 1970s and 1980s, mainly in the United States.[49] Only of a few of these compounds were widely used including rolicyclidine (PCPy), eticyclidine (PCE), and tenocyclidine (TCP).[49] Less common analogs include 3-HO-PCP, 3-MeO-PCMo, and 3-MeO-PCP.
The generalized structural motif required for PCP-like activity is derived from structure-activity relationship studies of PCP derivatives. All of these derivatives are likely to share some of their psychoactive effects with PCP itself, although a range of potencies and varying mixtures of anesthetic, dissociative, and stimulant effects are known, depending on the particular drug and its substituents. In some countries such as the United States, Australia, and New Zealand, all of these compounds would be considered controlled substance analogs of PCP under the Federal Analog Act and are hence illegal drugs if sold for human consumption.[74][75]
History edit
Phencyclidine was initially discovered in 1926 by Arthur Kötz and his student Paul Merkel as a product of a Grignard reaction of 1-piperidinocyclohexancarbonitrile.[76]
It was again made in 1956 and brought to market as an anesthetic medication.[72][11][77][76][78] Its use in humans was disallowed in the United States in 1965 due to the high rates of side effects, while its use in animals was disallowed in 1978.[1][11][79] Moreover, ketamine was discovered and was better tolerated as an anesthetic.[79]
PCP is classified as a schedule II drug in the United States.[1] A number of derivatives of PCP have been sold for recreational and non-medical use.[49]
Society and culture edit
Regulation edit
PCP is a Schedule II substance in the United States and its ACSCN is 7471.[80] Its manufacturing quota for 2014 was 19 grams.[81]
It is a Schedule I drug by the Controlled Drugs and Substances act in Canada, a List I drug of the Opium Law in the Netherlands, and a Class A substance in the United Kingdom.[82]
Frequency of use edit
PCP began to emerge as a recreational drug in major cities in the United States in the 1960s.[8] In 1978, People magazine and Mike Wallace of 60 Minutes called PCP the country's "number one" drug problem. Although recreational use of the drug had always been relatively low, it began declining significantly in the 1980s. In surveys, the number of high school students admitting to trying PCP at least once fell from 13% in 1979 to less than 3% in 1990.[19]: 46–49
Cultural depictions edit
Jean-Michel Basquiat depicted two angel dust users in his 1982 painting Dustheads.[83]
In Vivienne Medrano's adult animated musical comedy television series Hazbin Hotel, Angel Dust is an adult film star in Hell and one of the main protagonists.[84] He is known to struggle with addiction to phencyclidine, currently and during his time on earth. Additionally his canon cause of death is overdose by phencyclidine, naming himself after the drug.[85]
References edit
- ^ a b c d e "PCP Fast Facts". National Drug Intelligence Center. 2003. Archived from the original on 14 August 2021. Retrieved 19 February 2018.
- ^ Stobo JD, Traill TA, Hellmann DB, Ladenson PW, Petty BG (1996). The Principles and Practice of Medicine. McGraw Hill Professional. p. 933. ISBN 9780071383653.
high abuse liability
- ^ a b c d Malenka RC, Nestler EJ, Hyman SE (2009). "Chapter 15: Reinforcement and Addictive Disorders". In Sydor A, Brown RY (eds.). Molecular Neuropharmacology: A Foundation for Clinical Neuroscience (2nd ed.). New York: McGraw-Hill Medical. pp. 374–375. ISBN 9780071481274.
- ^ Stobo JD, Traill TA, Hellmann DB, Ladenson PW, Petty BG (1996). The Principles and Practice of Medicine. McGraw Hill Professional. p. 933. ISBN 9780071383653.
high abuse liability
- ^ a b c d e f g Giannini AJ (1998). "Chapter 35: Phencyclidine". In Tarter RE, Ammerman R, Ott PJ (eds.). Handbook of Substance Abuse: Neurobehavioral Pharmacology. New York: Plenum Publishing Corporation. pp. 579–587. ISBN 978-1-4757-2913-9.
- ^ a b c "NIDA InfoFacts: Hallucinogens – LSD, Peyote, Psilocybin, and PCP". National Institute on Drug Abuse. Retrieved 2018-02-19.
- ^ a b Riviello RJ (2010). Manual of forensic emergency medicine : a guide for clinicians. Sudbury, Mass.: Jones and Bartlett Publishers. pp. 41–42. ISBN 9780763744625.
- ^ a b c d e Bush DM (2013). "Emergency Department Visits Involving Phencyclidine (PCP)". The CBHSQ Report. Rockville (MD): Substance Abuse and Mental Health Services Administration (US). PMID 27656747.
PCP can lead to hostile behavior that may result in episodes of extreme violence
- ^ a b c "Hallucinogens". National Institute on Drug Abuse. January 2016. Retrieved 20 February 2018.
- ^ a b Marion NE, Oliver WM (2014). Drugs in American Society: An Encyclopedia of History, Politics, Culture, and the Law [3 volumes]. ABC-CLIO. p. 732. ISBN 9781610695961.
- ^ a b c Zedeck BE, Zedeck MS (2007). Forensic Pharmacology. Infobase Publishing. p. 97. ISBN 9781438103822.
- ^ "GINAD". www.ginad.org. Archived from the original on 2018-09-10. Retrieved 2018-02-20.
- ^ "PCP". CESAR. Archived from the original on 12 March 2010. Retrieved 20 February 2018.
- ^ "Hallucinogens". NIAD. Archived from the original on 3 June 2020. Retrieved 20 February 2018.
- ^ Millan MJ, Brocco M, Gobert A, Joly F, Bervoets K, Rivet J, et al. (December 1999). "Contrasting mechanisms of action and sensitivity to antipsychotics of phencyclidine versus amphetamine: importance of nucleus accumbens 5-HT2A sites for PCP-induced locomotion in the rat". The European Journal of Neuroscience. 11 (12): 4419–32. doi:10.1046/j.1460-9568.1999.00858.x. PMID 10594669. S2CID 43150509.
- ^ a b Diaz, Jaime. How Drugs Influence Behavior. Englewood Cliffs: Prentice Hall, 1996.
- ^ Chudler EM. "Neuroscience for Kids – PCP". Neuroscience for Kids. Retrieved 2011-01-26.
- ^ a b c d Bey T, Patel A (February 2007). "Phencyclidine intoxication and adverse effects: a clinical and pharmacological review of an illicit drug". The California Journal of Emergency Medicine. 8 (1): 9–14. PMC 2859735. PMID 20440387.
- ^ a b c d Inciardi JA (1992). The War on Drugs II. Mayfield Publishing Company. ISBN 978-1-55934-016-8.
- ^ a b Morgan JP, Kagan D (July 1980). "The Dusting of America: The Image of Phencyclidine (PCP) in the Popular Media". Journal of Psychedelic Drugs. 12 (3–4): 195–204. doi:10.1080/02791072.1980.10471426. PMID 7431414.
- ^ Brecher M, Wang BW, Wong H, Morgan JP (December 1988). "Phencyclidine and violence: clinical and legal issues". Journal of Clinical Psychopharmacology. 8 (6): 397–401. doi:10.1097/00004714-198812000-00003. PMID 3069880. S2CID 33659160.
- ^ Wish ED (1986). "PCP and crime: just another illicit drug?". NIDA Research Monograph. 64: 174–89. PMID 3086733.
- ^ Uchida M, Hida H, Mori K, Yoshimi A, Kitagaki S, Yamada K, et al. (August 2019). "Functional roles of the glial glutamate transporter (GLAST) in emotional and cognitive abnormalities of mice after repeated phencyclidine administration". Eur Neuropsychopharmacol. 29 (8): 918–24. doi:10.1016/j.euroneuro.2019.06.005. PMID 31303267. S2CID 195887087.
- ^ Luisada PV (August 1978). Petersen RC, Stillman RC (eds.). "The phencyclidine psychosis: phenomenology and treatment" (PDF). NIDA Research Monograph (21). National Institute on Drug Abuse: 241–253. PMID 101872.
- ^ Pender JW (October 1972). "Dissociative anesthesia". California Medicine. 117 (4): 46–47. PMC 1518731. PMID 18730832.
- ^ Giannini AJ (1997). Drugs of Abuse (Second ed.). Los Angeles: Practice Management Information Corp. p. 126. ISBN 978-1-57066-053-5.
- ^ Nestler EJ (October 12, 2008). "Review. Transcriptional mechanisms of addiction: role of DeltaFosB". Philos. Trans. R. Soc. Lond. B Biol. Sci. 363 (1507): 3245–3255. doi:10.1098/rstb.2008.0067. PMC 2607320. PMID 18640924.Nestler EJ (October 2008). "Table 1: Drugs of abuse known to induce ΔFosB in nucleus accumbens after chronic administration". Philos. Trans. R. Soc. Lond. B Biol. Sci. 363 (1507): 3245–55. doi:10.1098/rstb.2008.0067. PMC 2607320. PMID 18640924.
- ^ Noda Y, Nabeshima T (September 1998). "Neuronal mechanisms of phencyclidine-induced place aversion and preference in the conditioned place preference task". Methods and Findings in Experimental and Clinical Pharmacology. 20 (7): 607–11. doi:10.1358/mf.1998.20.7.485726. PMID 9819806.
- ^ Murrie B, Lappin J, Large M, Sara G (April 2020). "Transition of Substance-Induced, Brief, and Atypical Psychoses to Schizophrenia: A Systematic Review and Meta-analysis". Schizophrenia Bulletin. 46 (3): 505–516. doi:10.1093/schbul/sbz102. PMC 7147575. PMID 31618428.
- ^ a b c d Bertron JL, Seto M, Lindsley CW (October 2018). "DARK Classics in Chemical Neuroscience: Phencyclidine (PCP)". ACS Chemical Neuroscience. 9 (10): 2459–2474. doi:10.1021/acschemneuro.8b00266. PMID 29953199. S2CID 49603581.
- ^ "Fry Fast Facts". National Drug Intelligence Center. Archived from the original on 2021-04-17. Retrieved 2017-01-15.
- ^ a b c d Helman RS, Habal R (October 6, 2008). "Phencyclidine Toxicity". eMedicine. Retrieved on November 3, 2008.
- ^ a b c d Olmedo R (2002). "Chapter 69: Phencyclidine and ketamine". In Goldfrank LR, Flomenbaum NE, Lewin NA, Howland MA, Hoffman RS, Nelson LS (eds.). Goldfrank's Toxicologic Emergencies. New York: McGraw-Hill. pp. 1034–1041. ISBN 978-0-07-136001-2.
- ^ a b c Milhorn HT (Apr 1991). "Diagnosis and management of phencyclidine intoxication". American Family Physician. 43 (4): 1293–302. PMID 2008817.
- ^ Giannini AJ, Price WA (1985). "PCP: Management of acute intoxication". Medical Times. 113 (9): 43–49.
- ^ Giannini AJ, Eighan MS, Loiselle RH, Giannini MC (Apr 1984). "Comparison of haloperidol and chlorpromazine in the treatment of phencyclidine psychosis". Journal of Clinical Pharmacology. 24 (4): 202–4. doi:10.1002/j.1552-4604.1984.tb01831.x. PMID 6725621. S2CID 42278510.
- ^ Roth BL, Driscol J. "PDSP Ki Database". Psychoactive Drug Screening Program (PDSP). University of North Carolina at Chapel Hill and the United States National Institute of Mental Health. Retrieved 14 August 2017.
- ^ Berton JL, Seto M, Lindsley CW (June 2018). "DARK Classics in Chemical Neuroscience: Phencyclidine (PCP)". ACS Chem Neurosci. 9 (10): 2459–2474. doi:10.1021/acschemneuro.8b00266. PMID 29953199. S2CID 49603581.
- ^ a b c d e f g h i j k l m n o p q r Roth BL, Gibbons S, Arunotayanun W, Huang XP, Setola V, Treble R, et al. (2013). "The ketamine analogue methoxetamine and 3- and 4-methoxy analogues of phencyclidine are high affinity and selective ligands for the glutamate NMDA receptor". PLOS ONE. 8 (3): e59334. Bibcode:2013PLoSO...859334R. doi:10.1371/journal.pone.0059334. PMC 3602154. PMID 23527166.
- ^ a b c Rothman RB (1994). "PCP site 2: a high affinity MK-801-insensitive phencyclidine binding site". Neurotoxicol Teratol. 16 (4): 343–53. doi:10.1016/0892-0362(94)90022-1. PMID 7968938.
- ^ Frohlich J, Van Horn JD (2014). "Reviewing the ketamine model for schizophrenia". J. Psychopharmacol. (Oxford). 28 (4): 287–302. doi:10.1177/0269881113512909. PMC 4133098. PMID 24257811.
- ^ Seeman P, Guan HC (2008). "Phencyclidine and glutamate agonist LY379268 stimulate dopamine D2High receptors: D2 basis for schizophrenia". Synapse. 62 (11): 819–28. doi:10.1002/syn.20561. PMID 18720422. S2CID 206519749.
- ^ a b Kapur S, Seeman P (2002). "NMDA receptor antagonists ketamine and PCP have direct effects on the dopamine D(2) and serotonin 5-HT(2)receptors-implications for models of schizophrenia". Mol. Psychiatry. 7 (8): 837–44. doi:10.1038/sj.mp.4001093. PMID 12232776.
- ^ a b c Seeman P, Guan HC, Hirbec H (2009). "Dopamine D2High receptors stimulated by phencyclidines, lysergic acid diethylamide, salvinorin A, and modafinil". Synapse. 63 (8): 698–704. doi:10.1002/syn.20647. PMID 19391150. S2CID 17758902.
- ^ Rabin RA, Doat M, Winter JC (2000). "Role of serotonergic 5-HT2A receptors in the psychotomimetic actions of phencyclidine". Int. J. Neuropsychopharmacol. 3 (4): 333–338. doi:10.1017/S1461145700002091. PMID 11343613.
- ^ a b c d Goodman CB, Thomas DN, Pert A, Emilien B, Cadet JL, Carroll FI, et al. (1994). "RTI-4793-14, a new ligand with high affinity and selectivity for the (+)-MK801-insensitive [3H]1-]1-(2-thienyl)cyclohexyl]piperidine binding site (PCP site 2) of guinea pig brain". Synapse. 16 (1): 59–65. doi:10.1002/syn.890160107. PMID 8134901. S2CID 19829696.
- ^ Large CH, Bison S, Sartori I, Read KD, Gozzi A, Quarta D, et al. (Jul 2011). "The efficacy of sodium channel blockers to prevent phencyclidine-induced cognitive dysfunction in the rat: potential for novel treatments for schizophrenia". The Journal of Pharmacology and Experimental Therapeutics. 338 (1): 100–13. doi:10.1124/jpet.110.178475. PMID 21487071. S2CID 1862326.
- ^ Anis NA, Berry SC, Burton NR, D. Lodge (1983). "The dissociative anaesthetics, ketamine and phencyclidine, selectively reduce excitation of central mammalian neurones by N-methyl-aspartate". British Journal of Pharmacology. 79 (2): 565–575. doi:10.1111/j.1476-5381.1983.tb11031.x. PMC 2044888. PMID 6317114.
- ^ a b c d Morris H, Wallach J (2014). "From PCP to MXE: a comprehensive review of the non-medical use of dissociative drugs". Drug Testing and Analysis. 6 (7–8): 614–32. doi:10.1002/dta.1620. PMID 24678061.
- ^ Caddy C, Giaroli G, White TP, Shergill SS, Tracy DK (Apr 2014). "Ketamine as the prototype glutamatergic antidepressant: pharmacodynamic actions, and a systematic review and meta-analysis of efficacy". Therapeutic Advances in Psychopharmacology. 4 (2): 75–99. doi:10.1177/2045125313507739. PMC 3952483. PMID 24688759.
- ^ Klockgether T, Turski L, Schwarz M, Sontag KH, Lehmann J (Oct 1988). "Paradoxical convulsant action of a novel non-competitive N-methyl-D-aspartate (NMDA) antagonist, tiletamine". Brain Research. 461 (2): 343–8. doi:10.1016/0006-8993(88)90265-X. PMID 2846121. S2CID 41671395.
- ^ Burns JM, Boyer EW (2013). "Antitussives and substance abuse". Substance Abuse and Rehabilitation. 4: 75–82. doi:10.2147/SAR.S36761. PMC 3931656. PMID 24648790.
- ^ Aguayo LG, Warnick JE, Maayani S, Glick SD, Weinstein H, Albuquerque EX (May 1982). "Site of action of phencyclidine. IV. Interaction of phencyclidine and its analogues on ionic channels of the electrically excitable membrane and nicotinic receptor: implications for behavioral effects". Molecular Pharmacology. 21 (3): 637–47. PMID 6287200.
- ^ Zarantonello P, Bettini E, Paio A, Simoncelli C, Terreni S, Cardullo F (Apr 2011). "Novel analogues of ketamine and phencyclidine as NMDA receptor antagonists". Bioorganic & Medicinal Chemistry Letters. 21 (7): 2059–63. doi:10.1016/j.bmcl.2011.02.009. PMID 21334205.
- ^ Lin H, Vicini S, Hsu FC, Doshi S, Takano H, Coulter DA, et al. (Sep 2010). "Axonal α7 nicotinic ACh receptors modulate presynaptic NMDA receptor expression and structural plasticity of glutamatergic presynaptic boutons". Proceedings of the National Academy of Sciences of the United States of America. 107 (38): 16661–6. Bibcode:2010PNAS..10716661L. doi:10.1073/pnas.1007397107. PMC 2944730. PMID 20817852.
- ^ Fisher JL, Dani JA (Oct 2000). "Nicotinic receptors on hippocampal cultures can increase synaptic glutamate currents while decreasing the NMDA-receptor component". Neuropharmacology. 39 (13): 2756–69. doi:10.1016/s0028-3908(00)00102-7. PMID 11044745. S2CID 42066117.
- ^ Prestori F, Bonardi C, Mapelli L, Lombardo P, Goselink R, De Stefano ME, et al. (2013). "Gating of long-term potentiation by nicotinic acetylcholine receptors at the cerebellum input stage". PLOS ONE. 8 (5): e64828. Bibcode:2013PLoSO...864828P. doi:10.1371/journal.pone.0064828. PMC 3669396. PMID 23741401.
- ^ Seeman P, Ko F, Tallerico T (Sep 2005). "Dopamine receptor contribution to the action of PCP, LSD and ketamine psychotomimetics". Molecular Psychiatry. 10 (9): 877–83. doi:10.1038/sj.mp.4001682. PMID 15852061.
- ^ Giannini AJ, Nageotte C, Loiselle RH, Malone DA, Price WA (1984). "Comparison of chlorpromazine, haloperidol and pimozide in the treatment of phencyclidine psychosis: DA-2 receptor specificity". Journal of Toxicology. Clinical Toxicology. 22 (6): 573–9. doi:10.3109/15563658408992586. PMID 6535849.
- ^ Rothman RB, Reid AA, Monn JA, Jacobson AE, Rice KC (Dec 1989). "The psychotomimetic drug phencyclidine labels two high affinity binding sites in guinea pig brain: evidence for N-methyl-D-aspartate-coupled and dopamine reuptake carrier-associated phencyclidine binding sites". Molecular Pharmacology. 36 (6): 887–96. PMID 2557536.
- ^ Castellani S, Giannini AJ, Adams PM (1982). "Effects of naloxone, metenkephalin, and morphine on phencyclidine-induced behavior in the rat". Psychopharmacology. 78 (1): 76–80. doi:10.1007/BF00470593. PMID 6815700. S2CID 21996319.
- ^ "Phencyclidine". www.drugbank.ca. Retrieved 28 January 2019.
- ^ Martin D, Lodge D (October 1988). "Phencyclidine receptors and N-methyl-D-aspartate antagonism: electrophysiologic data correlates with known behaviours". Pharmacology, Biochemistry, and Behavior. 31 (2): 279–286. doi:10.1016/0091-3057(88)90346-2. PMID 2854262. S2CID 12247783.
- ^ a b Kohrs R, Durieux ME (November 1998). "Ketamine: teaching an old drug new tricks". Anesthesia and Analgesia. 87 (5): 1186–1193. doi:10.1097/00000539-199811000-00039. PMID 9806706.
- ^ Kroemer RT, Koutsilieri E, Hecht P, Liedl KR, Riederer P, Kornhuber J (January 1998). "Quantitative analysis of the structural requirements for blockade of the N-methyl-D-aspartate receptor at the phencyclidine binding site". Journal of Medicinal Chemistry. 41 (3): 393–400. doi:10.1021/jm9704412. PMID 9464369.
- ^ Nadler V, Kloog Y, Sokolovsky M (March 1990). "Distinctive structural requirement for the binding of uncompetitive blockers (phencyclidine-like drugs) to the NMDA receptor". European Journal of Pharmacology. 188 (2–3): 97–104. doi:10.1016/0922-4106(90)90044-X. PMID 2156715.
- ^ Olney JW, Labruyere J, Price MT (June 1989). "Pathological changes induced in cerebrocortical neurons by phencyclidine and related drugs". Science. 244 (4910): 1360–1362. Bibcode:1989Sci...244.1360O. doi:10.1126/science.2660263. PMID 2660263.
- ^ Hargreaves RJ, Hill RG, Iversen LL (1994). "Neuroprotective NMDA Antagonists: The Controversy over Their Potential for Adverse Effects on Cortical Neuronal Morphology". Brain Edema IX. Acta Neurochirurgica. Supplementum. Vol. 60. pp. 15–19. doi:10.1007/978-3-7091-9334-1_4. ISBN 978-3-7091-9336-5. PMID 7976530.
- ^ Jansen, Karl. Ketamine: Dreams and Realities. MAPS, 2004. ISBN 0-9660019-7-4
- ^ Reynolds LM, Cochran SM, Morris BJ, Pratt JA, Reynolds GP (March 2005). "Chronic phencyclidine administration induces schizophrenia-like changes in N-acetylaspartate and N-acetylaspartylglutamate in rat brain". Schizophrenia Research. 73 (2–3): 147–152. doi:10.1016/j.schres.2004.02.003. PMID 15653257. S2CID 1651693.
- ^ Murray JB (May 2002). "Phencyclidine (PCP): a dangerous drug, but useful in schizophrenia research". The Journal of Psychology. 136 (3): 319–327. doi:10.1080/00223980209604159. PMID 12206280. S2CID 20334137.
- ^ a b Lodge D, Mercier MS (September 2015). "Ketamine and phencyclidine: the good, the bad and the unexpected". British Journal of Pharmacology. 172 (17): 4254–4276. doi:10.1111/bph.13222. PMC 4556466. PMID 26075331.
- ^ Javitt DC, Zukin SR, Heresco-Levy U, Umbricht D (September 2012). "Has an angel shown the way? Etiological and therapeutic implications of the PCP/NMDA model of schizophrenia". Schizophrenia Bulletin. 38 (5): 958–966. doi:10.1093/schbul/sbs069. PMC 3446214. PMID 22987851.
- ^ Itzhak Y, Kalir A, Weissman BA, Cohen S (May 1981). "New analgesic drugs derived from phencyclidine". Journal of Medicinal Chemistry. 24 (5): 496–9. doi:10.1021/jm00137a004. PMID 7241506.
- ^ Chaudieu I, Vignon J, Chicheportiche M, Kamenka JM, Trouiller G, Chicheportiche R (Mar 1989). "Role of the aromatic group in the inhibition of phencyclidine binding and dopamine uptake by PCP analogs". Pharmacology Biochemistry and Behavior. 32 (3): 699–705. doi:10.1016/0091-3057(89)90020-8. PMID 2544905. S2CID 7672918.
- ^ a b Kötz A, Merkel P (May 1926). "Zur Kenntnis hydroaromatischer Alkamine". Journal für Praktische Chemie (in German). 113 (1): 49–76. doi:10.1002/prac.19261130107. ISSN 0021-8383.
- ^ Bunney Jr WE, Hippius H, Laakmann G, Schmauß M (2012). Neuropsychopharmacology: Proceedings of the XVIth C.I.N.P. Congress, Munich, August, 15-19, 1988. Springer Science & Business Media. p. 717. ISBN 978-3-642-74034-3.
- ^ Lindgren JE, Holmstedt B (1983). "Guide to the Analysis of Phencyclidine and its Metabolites in Biological Material". Toxicology in the Use, Misuse, and Abuse of Food, Drugs, and Chemicals. Archives of Toxicology. Vol. 6. Berlin, Heidelberg: Springer Berlin Heidelberg. pp. 61–73. doi:10.1007/978-3-642-69083-9_10. ISBN 978-3-540-12392-7. ISSN 0171-9750. PMID 6578750.
- ^ a b Tasman A, Kay J, Lieberman JA, First MB, Riba M (2015). Psychiatry, 2 Volume Set. John Wiley & Sons. p. 4943. ISBN 978-1-118-75336-1.
- ^ US Drug Enforcement Administration (March 12, 2014). "Controlled Substances" (PDF). Archived (PDF) from the original on 2014-04-17. Retrieved June 15, 2014.
- ^ US Drug Enforcement Administration (August 30, 2013). "Established Aggregate Production Quotas for Schedule I and II Controlled Substances and Established Assessment of Annual Needs for the List I Chemicals Ephedrine, Pseudoephedrine, and Phenylpropanolamine for 2014". Archived from the original on 2014-04-17. Retrieved June 15, 2014.
- ^ "The Misuse of Drugs Act 1971 (Modification) Order 1979". www.legislation.gov.uk. Retrieved 2016-01-31.
- ^ Nag A (April 11, 2013). "Christie's Evening Auction to present a major painting by Jean-Michel Basquiat". The Economic Times. Retrieved 2020-09-26.
- ^ "Prime Video Debuts Teaser of an Original Song and Announces Main Cast for Hazbin Hotel at New York Comic Con". press.amazonstudios.com. Retrieved 2024-02-22.
- ^ HAZBIN HOTEL Charity Sketch Request Stream Ft. Vivziepop, Cherri Bomb, and Angel Dust!. Retrieved 2024-02-22 – via YouTube.
External links edit
- Erowid.org – PCP Information
- National Institute of Drug Abuse InfoFacts: PCP (Phencyclidine) Archived 2012-01-06 at the Wayback Machine
- Drugs and Human Performance Fact Sheets on Phencyclidine
- Phencyclidine and Ketamine: A View From the Street-1981 article on the use and effects of PCP Archived 2019-01-21 at the Wayback Machine
- "Phencyclidine". Drug Information Portal. U.S. National Library of Medicine.