


Summary
The polyol pathway is a two-step process that converts glucose to fructose.[1] In this pathway glucose is reduced to sorbitol, which is subsequently oxidized to fructose. It is also called the sorbitol-aldose reductase pathway.
The pathway is implicated in diabetic complications, especially in microvascular damage to the retina,[2] kidney,[3] and nerves.[4]
Sorbitol cannot cross cell membranes, and, when it accumulates, it produces osmotic stresses on cells by drawing water into the insulin-independent tissues.[5]
Pathway edit
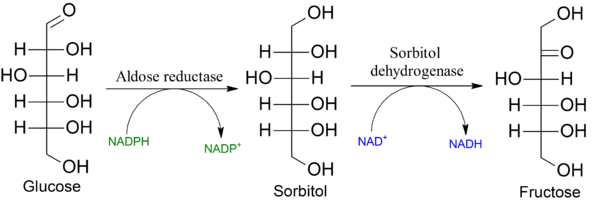
Cells use glucose for energy. This normally occurs by phosphorylation from the enzyme hexokinase. However, if large amounts of glucose are present (as in diabetes mellitus), hexokinase becomes saturated and the excess glucose enters the polyol pathway when aldose reductase reduces it to sorbitol. This reaction oxidizes NADPH to NADP+. Sorbitol dehydrogenase can then oxidize sorbitol to fructose, which produces NADH from NAD+. Hexokinase can return the molecule to the glycolysis pathway by phosphorylating fructose to form fructose-6-phosphate. However, in uncontrolled diabetics that have high blood glucose - more than the glycolysis pathway can handle - the reactions mass balance ultimately favors the production of sorbitol.[6]
Activation of the polyol pathway results in a decrease of reduced NADPH and oxidized NAD+; these are necessary co-factors in redox reactions throughout the body, and under normal conditions they are not interchangeable. The decreased concentration of these NADPH leads to decreased synthesis of reduced glutathione, nitric oxide, myo-inositol, and taurine. Myo-inositol is particularly required for the normal function of nerves. Sorbitol may also glycate nitrogens on proteins, such as collagen, and the products of these glycations are referred-to as AGEs - advanced glycation end-products. AGEs are thought to cause disease in the human body, one effect of which is mediated by RAGE (receptor for advanced glycation end-products) and the ensuing inflammatory responses induced. They are seen in the hemoglobin A1C tests performed on known diabetics to assess their levels of glucose control.[6]
Pathology edit
While most cells require the action of insulin for glucose to gain entry into the cell, the cells of the retina, kidney, and nervous tissues are insulin-independent, so glucose moves freely across the cell membrane, regardless of the action of insulin. The cells will use glucose for energy as normal, and any glucose not used for energy will enter the polyol pathway. When blood glucose is normal (about 100 mg/dL or 5.5 mmol/L), this interchange causes no problems, as aldose reductase has a low affinity for glucose at normal concentrations.[citation needed]
In a hyperglycemic state, the affinity of aldose reductase for glucose rises, causing much sorbitol to accumulate, and using much more NADPH, leaving less NADPH for other processes of cellular metabolism.[7] This change of affinity is what is meant by activation of the pathway. The amount of sorbitol that accumulates, however, may not be sufficient to cause osmotic influx of water.
NADPH acts to promote nitric oxide production and glutathione reduction, and its deficiency will cause glutathione deficiency. A glutathione deficiency, congenital or acquired, can lead to hemolysis caused by oxidative stress. Nitric oxide is one of the important vasodilators in blood vessels. Therefore, NADPH prevents reactive oxygen species from accumulating and damaging cells.[6]
Excessive activation of the polyol pathway increases intracellular and extracellular sorbitol concentrations, increased concentrations of reactive oxygen species, and decreased concentrations of nitric oxide and glutathione. Each of these imbalances can damage cells; in diabetes there are several acting together. It has not been conclusively determined that activating the polyol pathway damages the microvascular systems.[6]
References edit
- ^ Bonnefont-Rousselot D (September 2002). "Glucose and reactive oxygen species". Current Opinion in Clinical Nutrition and Metabolic Care. 5 (5): 561–8. doi:10.1097/00075197-200209000-00016. PMID 12172481. S2CID 20485164.
- ^ Behl T, Kaur I, Kotwani A (2016). "Implication of oxidative stress in progression of diabetic retinopathy". Survey of Ophthalmology. 61 (2): 187–96. doi:10.1016/j.survophthal.2015.06.001. PMID 26074354.
- ^ Forbes JM, Coughlan MT, Cooper ME (June 2008). "Oxidative stress as a major culprit in kidney disease in diabetes". Diabetes. 57 (6): 1446–54. doi:10.2337/db08-0057. PMID 18511445.
- ^ Javed S, Petropoulos IN, Alam U, Malik RA (January 2015). "Treatment of painful diabetic neuropathy". Therapeutic Advances in Chronic Disease. 6 (1): 15–28. doi:10.1177/2040622314552071. PMC 4269610. PMID 25553239.
- ^ Jedziniak JA, Chylack LT, Cheng HM, Gillis MK, Kalustian AA, Tung WH (March 1981). "The sorbitol pathway in the human lens: aldose reductase and polyol dehydrogenase". Investigative Ophthalmology & Visual Science. 20 (3): 314–26. PMID 6782033.
- ^ a b c d e Michael Brownlee (2005). "The pathobiology of diabetic complications: A unifying mechanism". Diabetes. 54 (6): 1615–1625. doi:10.2337/diabetes.54.6.1615. PMID 15919781.
- ^ Brownlee M (December 2001). "Biochemistry and molecular cell biology of diabetic complications". Nature. 414 (6865): 813–20. Bibcode:2001Natur.414..813B. doi:10.1038/414813a. PMID 11742414. S2CID 4396508.
Further references edit
- Harper's Illustrated Biochemistry(Published by LANGE)
- Dinesh Puri's Medical Biochemistry(Published by ELSEVIER)